Cromer Deborah, van Hoek Albert Jan, Newall Anthony T, Pollard Andrew J, Jit Mark
Kirby Institute for Infection and Immunity in Society, University of New South Wales, Sydney, NSW, Australia.
Department of Infectious Disease Epidemiology, London School of Hygiene & Tropical Medicine, London, UK.
Lancet Public Health. 2017 Jul 31;2(8):e367-e374. doi: 10.1016/S2468-2667(17)30103-2. eCollection 2017 Aug.
Vaccines and prophylactic antibodies against respiratory syncytial virus (RSV) are in development and likely to be available in the next 5-10 years. The most efficient way to use these products when they become available is an important consideration for public health decision makers.
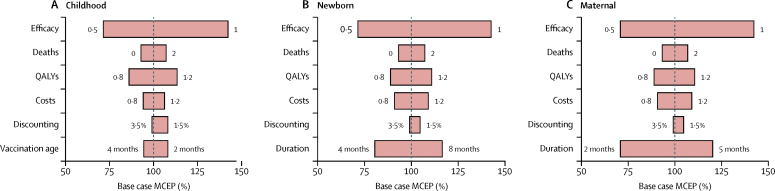
We performed a multivariate regression analysis to estimate the burden of RSV in children younger than 5 years in England (UK), a representative high-income temperate country, and used these results to assess the potential effect of different RSV immunisation strategies (targeting vaccination for infants, or pregnant women, or prophylactic antibodies for neonates). We did a cost-effectiveness analysis for these strategies, implemented either separately or concurrently, and assessed the effect of restricting vaccination to certain months of the year.
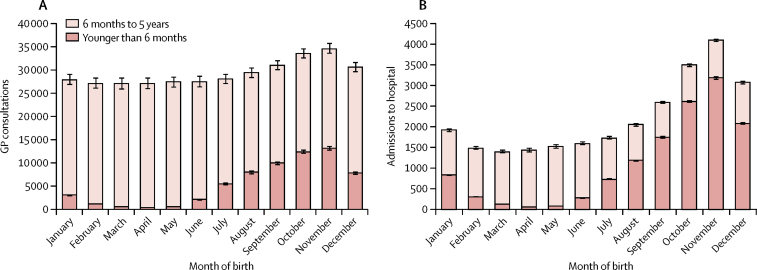
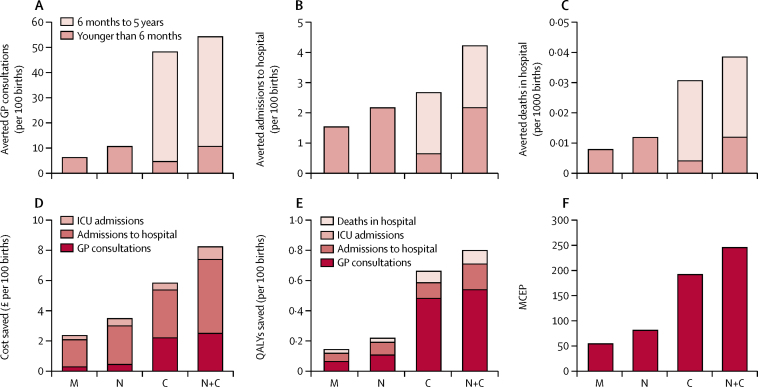
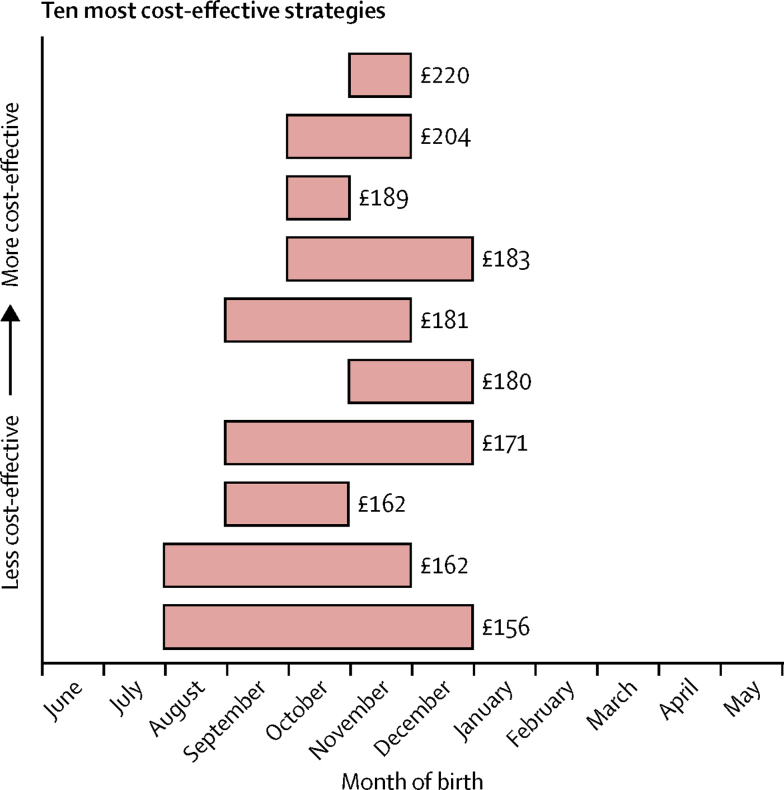
We estimated that RSV is responsible for 12 primary care consultations (95% CI 11·9-12·1) and 0·9 admissions to hospital annually per 100 children younger than 5 years (95% CI 0·89-0·90), with the major burden occurring in infants younger than 6 months. The most cost-effective strategy was to selectively immunise all children born before the start of the RSV season (maximum price of £220 [95% uncertainty interval (UI) 208-232] per vaccine, for an incremental cost-effectiveness ratio of £20 000 per quality-adjusted life-year). The maximum price per fully protected person that should be paid for the infant, newborn, and maternal strategies without seasonal restrictions was £192 (95% UI 168-219), £81 (76-86), and £54 (51-57), respectively.
Nearly double the number of primary care consultations, and nearly five times the number of admissions to hospital occurred with RSV compared with influenza. RSV vaccine and antibody strategies are likely to be cost-effective if they can be priced below around £200 per fully protected person. A seasonal vaccination strategy is likely to provide the most direct benefits. Herd effects might render a year-round infant vaccination strategy more appealing, although it is currently unclear whether such a programme would induce herd effects.
UK National Institute for Health Research.
针对呼吸道合胞病毒(RSV)的疫苗和预防性抗体正在研发中,未来5至10年内可能上市。这些产品上市后,如何以最有效的方式使用是公共卫生决策者需要重点考虑的问题。
我们进行了多变量回归分析,以估算英国(代表高收入温带国家)5岁以下儿童RSV的疾病负担,并利用这些结果评估不同RSV免疫策略(针对婴儿、孕妇接种疫苗,或为新生儿使用预防性抗体)的潜在效果。我们对这些单独或同时实施的策略进行了成本效益分析,并评估了将疫苗接种限制在一年中某些月份的效果。
我们估计,每100名5岁以下儿童中,RSV每年导致12次初级保健咨询(95%置信区间11.9 - 12.1)和0.9次住院(95%置信区间0.89 - 0.90),主要负担发生在6个月以下的婴儿中。最具成本效益的策略是选择性地为RSV季节开始前出生的所有儿童接种疫苗(每剂疫苗最高价格为220英镑[95%不确定区间(UI)208 - 232],每质量调整生命年的增量成本效益比为20000英镑)。对于无季节限制的婴儿、新生儿和孕产妇策略,每位完全受保护者应支付的最高价格分别为192英镑(95% UI 168 - 219)、81英镑(76 - 86)和54英镑(51 - 57)。
与流感相比,RSV导致的初级保健咨询次数几乎翻倍,住院次数几乎增加五倍。如果RSV疫苗和抗体策略的定价能低于每位完全受保护者约200英镑,那么它们可能具有成本效益。季节性疫苗接种策略可能会带来最直接的益处。群体效应可能会使全年婴儿疫苗接种策略更具吸引力,尽管目前尚不清楚这样的计划是否会引发群体效应。
英国国家卫生研究院。