Dutton Gareth R, Gowey Marissa A, Tan Fei, Zhou Dali, Ard Jamy, Perri Michael G, Lewis Cora E
Division of Preventive Medicine, Department of Medicine, University of Alabama at Birmingham, Birmingham, AL, USA.
Department of Mathematical Sciences, Indiana University-Purdue University Indianapolis, Indianapolis, IN, USA.
Int J Behav Nutr Phys Act. 2017 Aug 15;14(1):107. doi: 10.1186/s12966-017-0564-1.
Behavioral interventions for obesity produce clinically meaningful weight loss, but weight regain following treatment is common. Extended care programs attenuate weight regain and improve weight loss maintenance. However, less is known about the most effective ways to deliver extended care, including contact schedules.
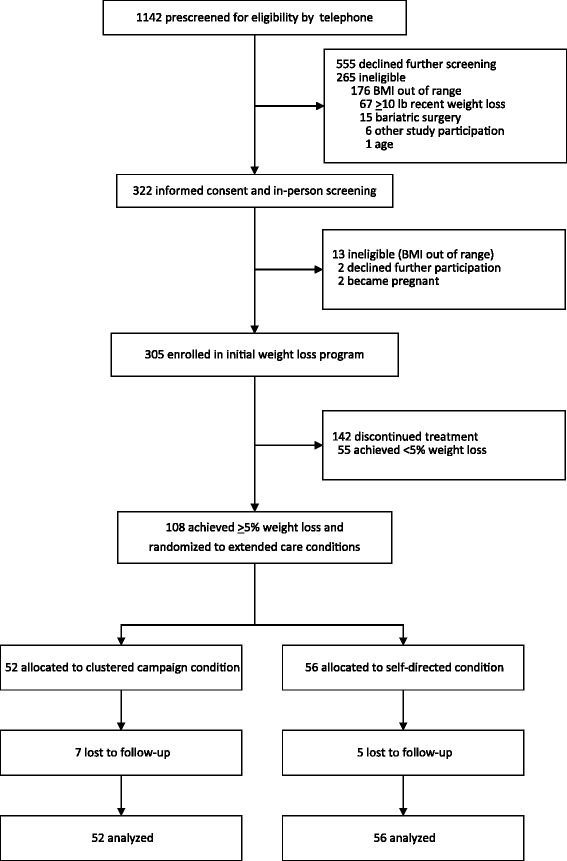
We compared the 12-month weight regain of an extended care program utilizing a non-conventional, clustered campaign treatment schedule and a self-directed program among individuals who previously achieved ≥5% weight reductions. Participants (N = 108; mean age = 51.6 years; mean weight = 92.6 kg; 52% African American; 95% female) who achieved ≥5% weight loss during an initial 16-week behavioral obesity treatment were randomized into a 2-arm, 12-month extended care trial. A clustered campaign condition included 12 group-based visits delivered in three, 4-week clusters. A self-directed condition included provision of the same printed intervention materials but no additional treatment visits. The study was conducted in a U.S. academic medical center from 2011 to 2015.
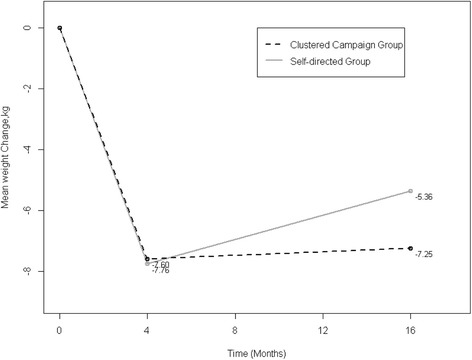
Prior to randomization, participants lost an average of -7.55 ± 3.04 kg. Participants randomized to the 12-month clustered campaign program regained significantly less weight (0.35 ± 4.62 kg) than self-directed participants (2.40 ± 3.99 kg), which represented a significant between-group difference of 2.28 kg (p = 0.0154) after covariate adjustments. This corresponded to maintaining 87% and 64% of lost weight in the clustered campaign and self-directed conditions, respectively, which was a significant between-group difference of 29% maintenance of lost weight after covariate adjustments, p = 0.0396.
In this initial test of a clustered campaign treatment schedule, this novel approach effectively promoted 12-month maintenance of lost weight. Future trials should directly compare the clustered campaigns with conventional (e.g., monthly) extended care schedules.
Clinicaltrials.gov NCT02487121 . Registered 06/26/2015 (retrospectively registered).
针对肥胖的行为干预可实现具有临床意义的体重减轻,但治疗后体重反弹很常见。延续性护理项目可减轻体重反弹并改善体重减轻的维持情况。然而,对于提供延续性护理的最有效方式,包括接触计划,人们了解较少。
我们比较了采用非常规、集中式活动治疗计划的延续性护理项目与自我指导项目在之前体重减轻≥5%的个体中的12个月体重反弹情况。在最初为期16周的行为性肥胖治疗中体重减轻≥5%的参与者(N = 108;平均年龄 = 51.6岁;平均体重 = 92.6千克;52%为非裔美国人;95%为女性)被随机分为两组,进行为期12个月的延续性护理试验。集中式活动组包括12次基于小组的访视,分三个为期4周的阶段进行。自我指导组包括提供相同的印刷干预材料,但没有额外的治疗访视。该研究于2011年至2015年在美国一家学术医疗中心进行。
在随机分组前,参与者平均体重减轻了-7.55±3.04千克。随机分配到为期12个月的集中式活动项目的参与者体重反弹(0.35±4.62千克)明显少于自我指导组参与者(2.40±3.99千克),经协变量调整后,组间差异显著,为2.28千克(p = 0.0154)。这分别相当于在集中式活动组和自我指导组中维持了87%和64%的减重效果,经协变量调整后,组间维持减重效果的差异显著,为29%,p = 0.0396。
在对集中式活动治疗计划的首次测试中,这种新方法有效地促进了12个月的体重减轻维持情况。未来的试验应直接将集中式活动与传统(如每月一次)的延续性护理计划进行比较。
Clinicaltrials.gov NCT02487121。于2015年6月26日注册(追溯注册)。