Kenya Medical Research Institute-Wellcome Trust Research Programme, Nairobi, Kenya.
National Malaria Control Programme, Ministry of Health, Nairobi, Kenya.
Malar J. 2017 Aug 17;16(1):344. doi: 10.1186/s12936-017-1973-y.
Health facility-based data reported through routine health information systems form the primary data source for programmatic monitoring and evaluation in most developing countries. The adoption of District Health Information Software (DHIS2) has contributed to improved availability of routine health facility-based data in many low-income countries. An assessment of malaria indicators data reported by health facilities in Kenya during the first 5 years of implementation of DHIS2, from January 2011 to December 2015, was conducted.
Data on 19 malaria indicators reported monthly by health facilities were extracted from the online Kenya DHIS2 database. Completeness of reporting was analysed for each of the 19 malaria indicators and expressed as the percentage of data values actually reported over the expected number; all health facilities were expected to report data for each indicator for all 12 months in a year.
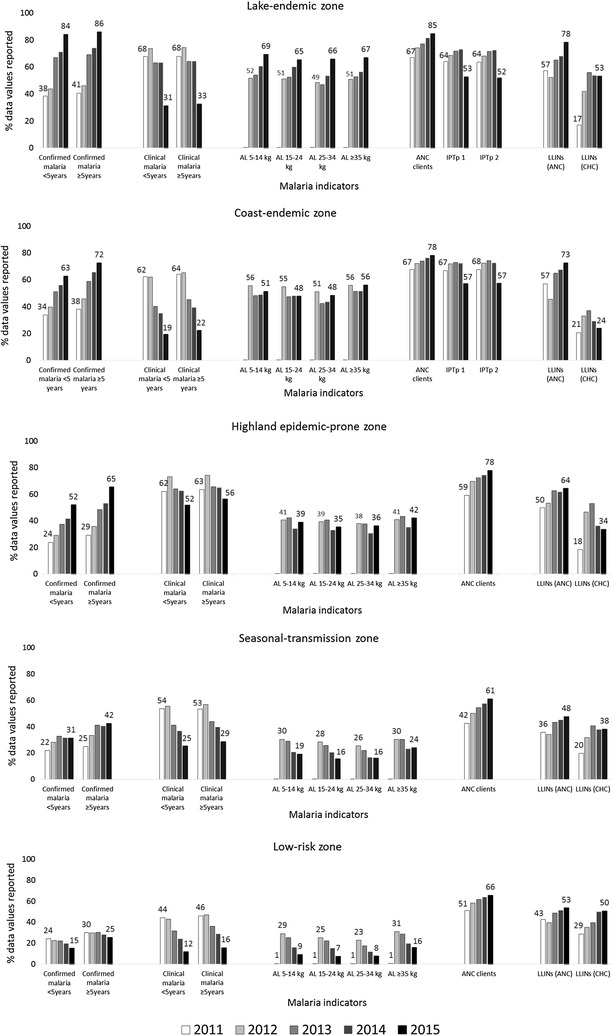
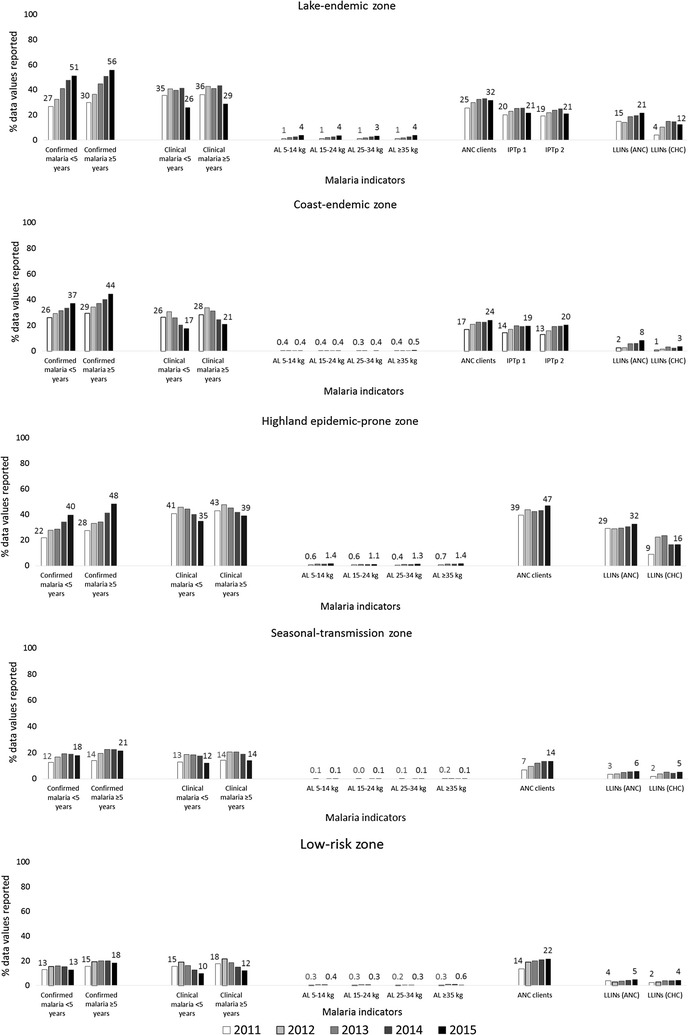
Malaria indicators data were analysed for 6235 public and 3143 private health facilities. Between 2011 and 2015, completeness of reporting in the public sector increased significantly for confirmed malaria cases across all age categories (26.5-41.9%, p < 0.0001, in children aged <5 years; 30.6-51.4%, p < 0.0001, in persons aged ≥5 years). Completeness of reporting of new antenatal care (ANC) clients increased from 53.7 to 70.5%, p < 0.0001). Completeness of reporting of intermittent preventive treatment in pregnancy (IPTp) decreased from 64.8 to 53.7%, p < 0.0001 for dose 1 and from 64.6 to 53.4%, p < 0.0001 for dose 2. Data on malaria tests performed and test results were not available in DHIS2 from 2011 to 2014. In 2015, sparse data on microscopy (11.5% for children aged <5 years; 11.8% for persons aged ≥5 years) and malaria rapid diagnostic tests (RDTs) (8.1% for all ages) were reported. In the private sector, completeness of reporting increased significantly for confirmed malaria cases across all age categories (16.7-23.1%, p < 0.0001, in children aged <5 years; 19.4-28.6%, p < 0.0001, in persons aged ≥5 years). Completeness of reporting also improved for new ANC clients (16.2-23.6%, p < 0.0001), and for IPTp doses 1 and 2 (16.6-20.2%, p < 0.0001 and 15.5-20.5%, p < 0.0001, respectively). In 2015, less than 3% of data values for malaria tests performed were reported in DHIS2 from the private sector.
There have been sustained improvements in the completeness of data reported for most key malaria indicators since the adoption of DHIS2 in Kenya in 2011. However, major data gaps were identified for the malaria-test indicator and overall low reporting across all indicators from private health facilities. A package of proven DHIS2 implementation interventions and performance-based incentives should be considered to improve private-sector data reporting.
在大多数发展中国家,基于卫生机构的卫生信息系统报告的数据是规划监测和评价的主要数据源。在许多低收入国家,采用地区卫生信息系统(DHIS2)有助于提高常规卫生机构数据的可用性。对肯尼亚在实施 DHIS2 的头 5 年(2011 年 1 月至 2015 年 12 月)期间卫生机构报告的疟疾指标数据进行了评估。
从在线肯尼亚 DHIS2 数据库中提取了 19 项每月由卫生机构报告的疟疾指标数据。分析了每个疟疾指标的报告完整性,并表示为实际报告的数据值与预期数据值之比;所有卫生机构均应在一年中的 12 个月内报告每个指标的数据。
分析了 6235 家公立和 3143 家私立卫生机构的疟疾指标数据。2011 年至 2015 年期间,公立部门报告的确诊疟疾病例完整性显著提高(所有年龄组 26.5-41.9%,p<0.0001,<5 岁儿童;30.6-51.4%,p<0.0001,≥5 岁人群)。新产前保健(ANC)客户的报告完整性从 53.7%增加到 70.5%(p<0.0001)。妊娠间歇性预防治疗(IPTp)的报告完整性从 64.8%下降到 53.7%(第 1 剂,p<0.0001)和 64.6%下降到 53.4%(第 2 剂,p<0.0001)。2011 年至 2014 年,DHIS2 中未提供疟疾检测和检测结果的数据。2015 年,仅报告了少量显微镜检查(<5 岁儿童 11.5%;≥5 岁人群 11.8%)和疟疾快速诊断检测(RDTs)(所有年龄段 8.1%)的数据。在私立部门,所有年龄组的确诊疟疾病例报告完整性均显著提高(<5 岁儿童 16.7-23.1%,p<0.0001;≥5 岁人群 19.4-28.6%,p<0.0001)。新 ANC 客户的报告完整性也得到了改善(16.2-23.6%,p<0.0001),第 1 和第 2 剂 IPTp 的报告完整性也得到了改善(16.6-20.2%,p<0.0001 和 15.5-20.5%,p<0.0001)。2015 年,DHIS2 中私立部门报告的疟疾检测数据值不到 3%。
自 2011 年肯尼亚采用 DHIS2 以来,大多数关键疟疾指标的数据报告完整性持续提高。然而,疟疾检测指标和整体低报告率仍然存在重大数据差距,所有私立卫生机构的所有指标均如此。应考虑实施经证实的 DHIS2 干预措施和基于绩效的激励措施,以改善私立部门的数据报告。