Schwartzberg Lee S, Arena Francis P, Bienvenu Bryan J, Kaplan Edward H, Camacho Luis H, Campos Luis T, Waymack J Paul, Tagliaferri Mary A, Chen Michael M, Li Dapeng
West Cancer Center, Germantown, TN.
Arena Oncology Associates, New York, NY.
J Cancer. 2017 Jul 3;8(10):1872-1883. doi: 10.7150/jca.15407. eCollection 2017.
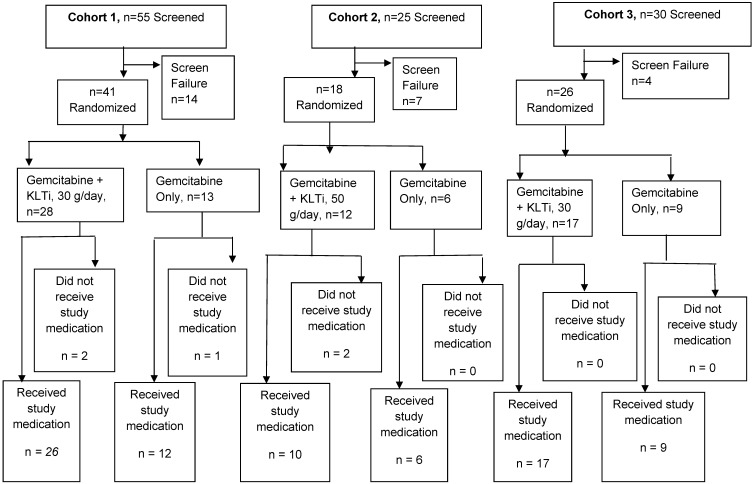
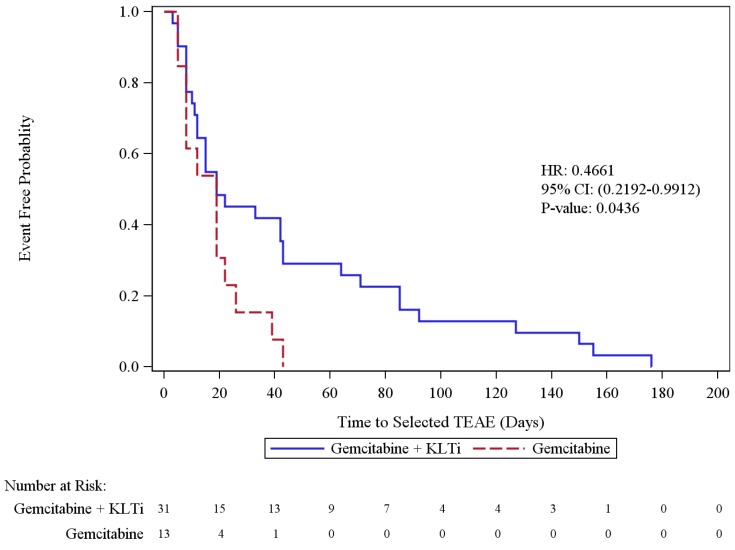
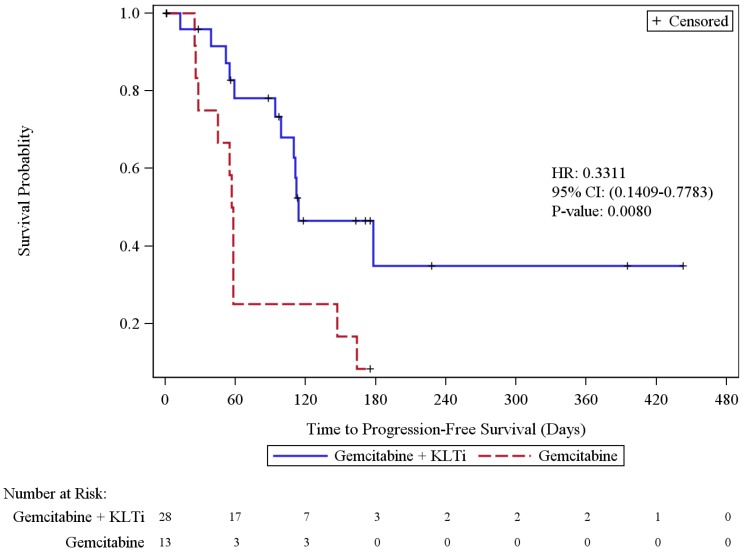
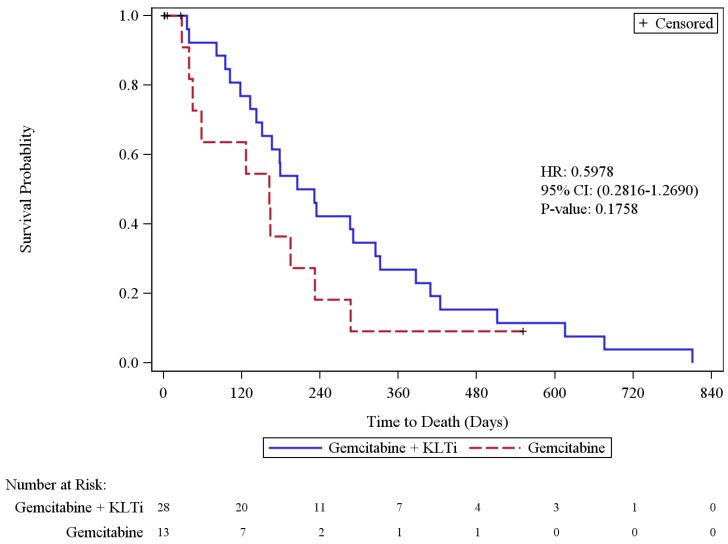
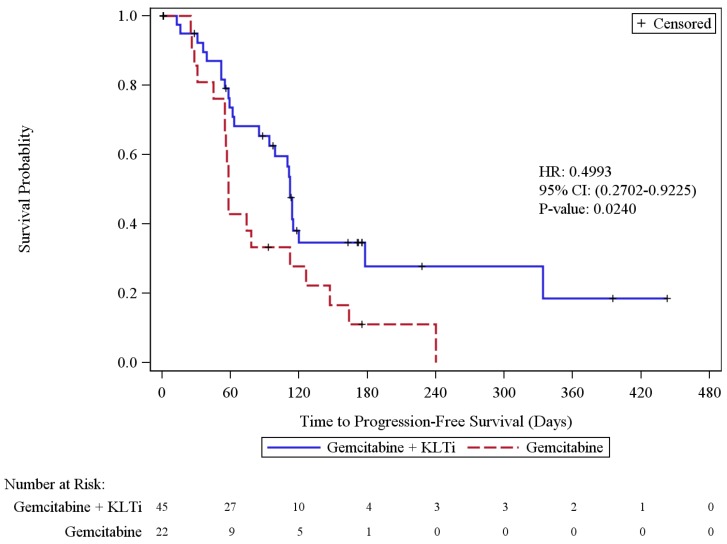
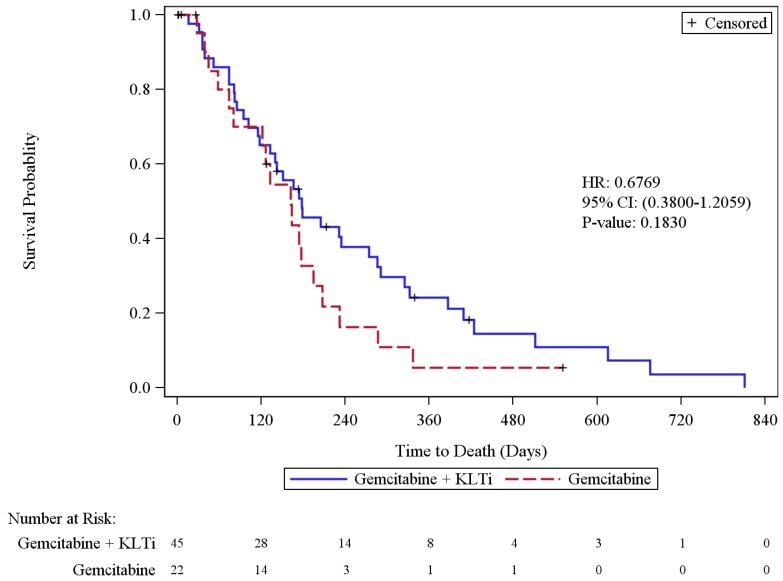
This study was designed to assess the safety and preliminary efficacy of KLTi plus gemcitabine in patients with locally advanced or metastatic pancreatic cancer. In a randomized, open-label study, patients with locally advanced or metastatic pancreatic cancer were randomized 2:1 to receive KLTi plus gemcitabine or gemcitabine monotherapy. Three sequential cohorts were tested at 30 g/day, 50 g/day, and 30 g/day. Gemcitabine was administered at 1000 mg/m on days 1, 8 and 15 of each 28 day cycle. KLTi was administered on days 1-5, 8-12, and 15-19 of each 28 day cycle. Patients received study treatment until disease progression. The primary endpoint was progression-free survival in the ITT population. Safety evaluation was based on patients who received any study treatment. ClinicalTrials.gov identifier NCT00733850. Eighty-five patients were randomized including 41 (28:13) in Cohort 1, 18 (12:6) in Cohort 2, and 26 (17:9) in Cohort 3. Due to a different dose and/or shift in patient populations in Cohort 2 and 3, efficacy data for the 30 gm dose are presented in this manuscript for Cohort 1 alone, and for the combination of Cohort 1+3. The 30 gm KLTi + gemcitabine group had a statistically significant improvement in progression-free survival (PFS) as assessed by blinded independent radiology review in the ITT population, with a median of 112 days, versus 58 days in the gemcitabine group (HR 0.50; 95% CI: 0.27, 0.92), p = 0.0240. The incidence rates of TEAEs, CTCAE Grade 3 or higher TEAEs, and SAEs were similar between the two arms. There were no deaths related to KLTi + gemcitabine treatment. Kanglaite Injection (30 g/day) plus a standard regimen of gemcitabine demonstrated encouraging clinical evidence of anti-neoplastic activity and a well-tolerated safety profile.
本研究旨在评估康莱特注射液(KLTi)联合吉西他滨治疗局部晚期或转移性胰腺癌患者的安全性和初步疗效。在一项随机、开放标签研究中,局部晚期或转移性胰腺癌患者按2:1随机分组,分别接受KLTi联合吉西他滨或吉西他滨单药治疗。三个连续队列分别按每日30 g、50 g和30 g进行测试。在每28天周期的第1、8和15天给予吉西他滨,剂量为1000 mg/m²。在每28天周期的第1 - 5天、8 - 12天和15 - 19天给予KLTi。患者接受研究治疗直至疾病进展。主要终点是意向性治疗(ITT)人群的无进展生存期。安全性评估基于接受任何研究治疗的患者。ClinicalTrials.gov标识符为NCT00733850。85例患者被随机分组,其中队列1有41例(28:13),队列2有18例(12:6),队列3有26例(17:9)。由于队列2和队列3的剂量不同和/或患者人群有变化,本手稿仅呈现队列1以及队列1 + 3组合中30 g剂量的疗效数据。经ITT人群中盲法独立放射学评估,30 g KLTi + 吉西他滨组的无进展生存期(PFS)有统计学显著改善,中位生存期为112天,而吉西他滨组为58天(风险比0.50;95%置信区间:0.27, 0.92),p = 0.0240。两组之间治疗期间出现的不良事件(TEAE)、3级或更高等级TEAE以及严重不良事件(SAE)的发生率相似。没有与KLTi + 吉西他滨治疗相关的死亡病例。康莱特注射液(每日30 g)联合吉西他滨标准方案显示出令人鼓舞的抗肿瘤活性临床证据,且安全性良好,耐受性佳。