C.T. Lamont Primary Healthcare Research Centre, Bruyère Research Institute, 43 Bruyere St, Annex E, Room 106, Ottawa, ON, K1N 5C8, Canada.
Department of Family Medicine, University of Ottawa, 75 Laurier Ave E, Ottawa, ON, Canada.
BMC Fam Pract. 2017 Aug 22;18(1):81. doi: 10.1186/s12875-017-0654-9.
In many countries, the referral-consultation process faces a number of challenges from inefficiencies and rising demand, resulting in excessive wait times for many specialties. We collected referral data from a sample of family doctors across the province of Ontario, Canada as part of a larger program of research. The purpose of this study is to describe referral patterns from primary care to specialist and allied health services from the primary care perspective.
We conducted a prospective study of patient referral data submitted by primary care providers (PCP) from 20 clinics across Ontario between June 2014 and January 2016. Monthly referral volumes expressed as a total number of referrals to all medical and allied health professionals per month. For each referral, we also collected data on the specialty type, reason for referral, and whether the referral was for a procedure.
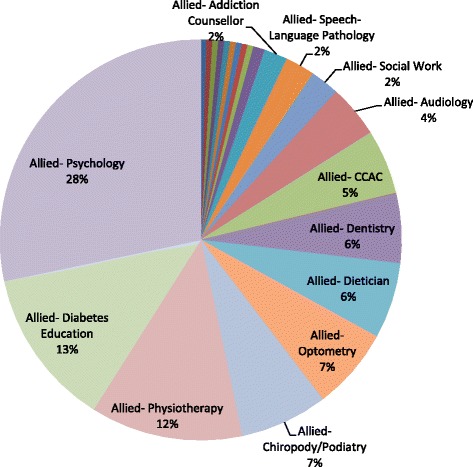
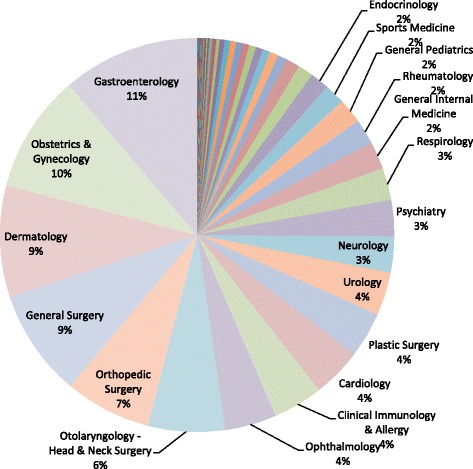
PCPs submitted a median of 26 referrals per month (interquartile range 11.5 to 31.8). Of 9509 referrals eligible for analysis, 97.8% were directed to medical professionals and 2.2% to allied health professionals. 55% of medical referrals were directed to non-surgical specialties and 44.8% to surgical specialties. Medical referrals were for procedures in 30.8% of cases and non-procedural in 40.9%. Gastroenterology received the largest share (11.2%) of medical referrals, of which 62.3% were for colonoscopies. Psychology received the largest share (28.3%) of referrals to allied health professionals.
We described patterns of patient referral from primary care to specialist and allied health services for 30 PCPs in 20 clinics across Ontario. Gastroenterology received the largest share of referrals, nearly two-thirds of which were for colonoscopies. Future studies should explore the use of virtual care to help manage non-procedural referrals and examine the impact that procedural referrals have on wait times for gastroenterology.
在许多国家,转诊-会诊流程面临着效率低下和需求上升带来的诸多挑战,导致许多专科的等待时间过长。我们从加拿大安大略省的一个样本家庭医生那里收集了转诊数据,作为一个更大的研究项目的一部分。本研究的目的是从初级保健的角度描述向专科和辅助卫生服务的转诊模式。
我们对 2014 年 6 月至 2016 年 1 月期间安大略省 20 家诊所的初级保健提供者(PCP)提交的患者转诊数据进行了前瞻性研究。每月转诊量表示每月转诊给所有医疗和辅助卫生专业人员的总人数。对于每一次转诊,我们还收集了专科类型、转诊原因以及转诊是否为程序的相关数据。
PCP 每月提交的中位数转诊量为 26 次(四分位距 11.5 至 31.8)。在 9509 次符合分析条件的转诊中,97.8%的转诊对象是医疗专业人员,2.2%的转诊对象是辅助卫生专业人员。55%的医疗转诊是指向非手术专科,44.8%的转诊是指向手术专科。在 30.8%的情况下,医疗转诊是为了程序,40.9%的转诊是非程序的。胃肠病学收到的医疗转诊比例最大(11.2%),其中 62.3%是结肠镜检查。心理学收到的转诊比例最大(28.3%),其中 28.3%是转诊给辅助卫生专业人员。
我们描述了安大略省 20 家诊所的 30 名初级保健医生向专科和辅助卫生服务的患者转诊模式。胃肠病学收到的转诊比例最大,其中近三分之二是结肠镜检查。未来的研究应该探索使用虚拟护理来帮助管理非程序转诊,并研究程序转诊对胃肠病学等待时间的影响。