Micic Dejan, Gaetano John N, Rubin Jonah N, Cohen Russell D, Sakuraba Atsushi, Rubin David T, Pekow Joel
Department of Internal Medicine, Section of Gastroenterology, Hepatology and Nutrition, University of Chicago, Chicago, Illinois, United States of America.
Department of Internal Medicine, Section of Hospital Medicine, University of Chicago, Chicago, Illinois, United States of America.
PLoS One. 2017 Aug 24;12(8):e0182900. doi: 10.1371/journal.pone.0182900. eCollection 2017.
Management of inpatients with inflammatory bowel disease (IBD) requires increasing resources. We aimed to identify factors associated with hospital readmissions among individuals with IBD.
MATERIALS & METHODS: We collected data from the Healthcare Cost and Utilization Project Nationwide Readmissions Database 2013. We identified individuals with index hospitalizations for IBD. Patient-specific factors, comorbidities and hospitalization characteristics were extracted for the index hospitalization. We performed logistic regression modeling to create adjusted odds ratios (ORs) for 30-day hospital readmission. Subgroup analysis was performed based on disease type and performance of surgery.
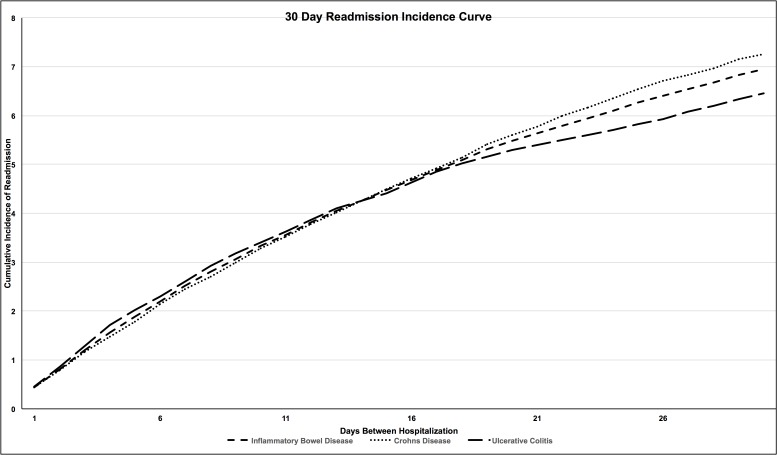
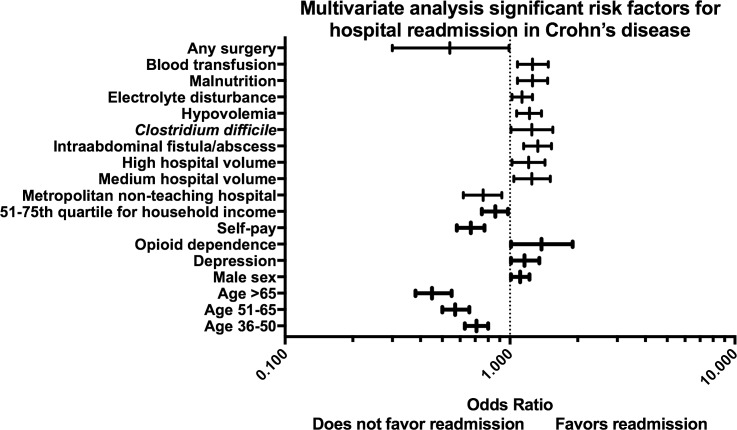
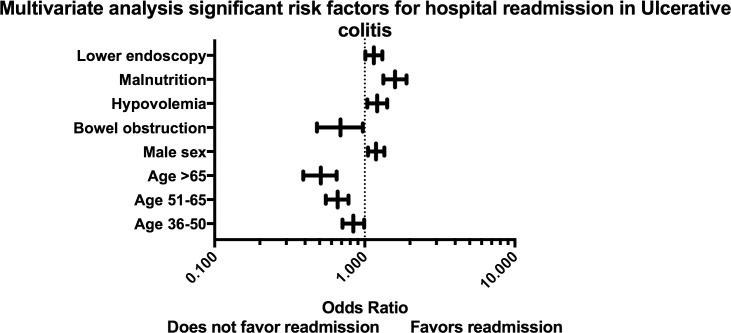
We analyzed a total of 55,942 index hospital discharges; 3037 patients (7.0%) were readmitted to the hospital within 30 days. Increasing patient age (> 65: OR: 0.45; 95% CI 0.39-0.53) was associated with a decreased risk of readmission, while a diagnosis of Crohn's disease (OR: 1.09; 95% CI 1.00-1.18) and male sex (OR: 1.16; 95% CI 1.07-1.25) were associated with an increased risk of readmission. The comorbidities of smoking (OR: 1.09; 95% CI 1.00-1.19), anxiety (OR: 1.17; 95% CI 1.01-1.36) and opioid dependence (OR: 1.40; 95% CI 1.06-1.86) were associated with an increased risk of 30-day readmission. Individual hospitalization characteristics and disease complications were significantly associated with readmission. Performance of a surgery during the index admission was associated with a decreased risk of readmission (OR: 0.57; 95% CI 0.33-0.96).
Analyzing data from a US publicly available all-payer inpatient healthcare database, we identified patient and hospitalization risk factors associated with 30-day readmission. Identifying patients at high risk for readmission may allow for interventions during or after the index hospitalization to decrease this risk.
炎症性肠病(IBD)住院患者的管理需要更多资源。我们旨在确定IBD患者再次入院的相关因素。
我们从2013年医疗成本和利用项目全国再入院数据库中收集数据。我们确定了因IBD首次住院的患者。提取了首次住院的患者特定因素、合并症和住院特征。我们进行了逻辑回归建模,以创建30天再次入院的调整比值比(OR)。根据疾病类型和手术情况进行亚组分析。
我们共分析了55942例首次出院病例;3037例患者(7.0%)在30天内再次入院。患者年龄增加(>65岁:OR:0.45;95%CI 0.39 - 0.53)与再次入院风险降低相关,而克罗恩病诊断(OR:1.09;95%CI 1.00 - 1.18)和男性(OR:1.16;95%CI 1.07 - 1.25)与再次入院风险增加相关。吸烟(OR:1.09;95%CI 1.00 - 1.19)、焦虑(OR:1.17;95%CI 1.01 - 1.36)和阿片类药物依赖(OR:1.40;95%CI 1.06 - 1.86)等合并症与30天再次入院风险增加相关。个体住院特征和疾病并发症与再次入院显著相关。首次住院期间进行手术与再次入院风险降低相关(OR:0.57;95%CI 0.33 - 0.96)。
通过分析美国公开可用的全付费者住院医疗数据库中的数据,我们确定了与30天再次入院相关的患者和住院风险因素。识别再次入院高风险患者可能有助于在首次住院期间或之后进行干预,以降低这种风险。