Ongwae Kennedy M, Bawa Samuel B, Shuaib Faisal, Braka Fiona, Corkum Melissa, Isa Hammanyero K
Health, United Nations Children's Fund (UNICEF), Islamabad, Pakistan.
Polio, World Health Organization.
J Infect Dis. 2017 Jul 1;216(suppl_1):S267-S272. doi: 10.1093/infdis/jiw520.
The Polio Eradication Initiative in Nigeria, which started >20 years ago, faced many challenges, including initial denial, resistance from communities, and prolonged regional safety concerns. These challenges led into the structuring of the response including the development of the National Emergency Action Plan, improved partner coordination and government engagement, and the establishment of a Polio Emergency Operations Centre. Although monthly supplementary immunization activities (SIAs) continued, the targeting of settlements at high risk for polio transmission with routine immunization (RI) and other selected primary healthcare (PHC) services using dedicated mobile teams and volunteer community mobilizers (VCMs) became a key strategy for interrupting polio transmission in the high-risk areas. These efforts could have contributed to the wild poliovirus-free 2-year period between 24 July 2014 and 11 August 2016, when 2 cases of the virus were reported from Borno State, Northern Nigeria.
A narrative analysis of polio-related program and other official documents was conducted to identify the relevant human resources and their role in the Polio Eradication Initiative and in RI. The data used in the article was obtained from United Nations Children's Fund (UNICEF) and World Health Organization project reports and a draft evaluation report of the dedicated mobile teams approach in Northern Nigeria.
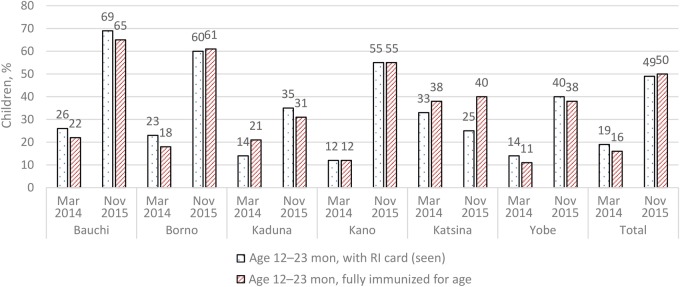
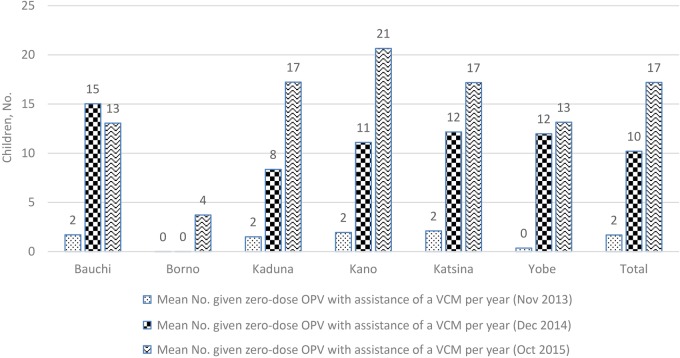
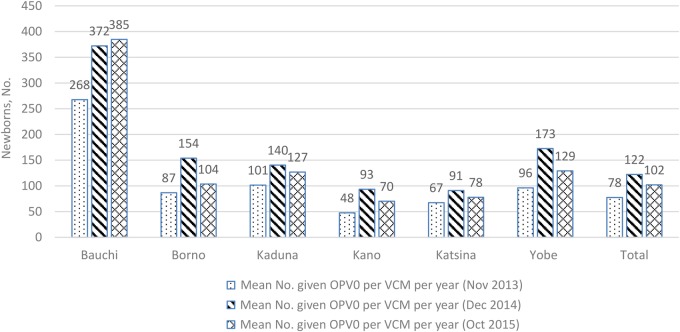
The data from 6 of the states that commenced the provision of polio, RI, and other selected PHC services using the dedicated mobile teams approach in 2014 showed an overall increase in the percentage of children aged 12-23 months in the settlements at high risk for polio transmission with a RI card seen, from 23% to 56%, and an overall increase in fully immunized children aged 12-23 months, from 19% to 55%. The number of newborns given the first dose of oral poliovirus vaccine (OPV) according to the RI schedule and the number of children given zero-dose OPV with the assistance of the VCMs similarly increased between 2013 and 2015. In 2015, VCMs helped track 167 092 newborns and also linked 156 537 infants aged <1 year to RI services in the 6 states.
The analysis illustrates that polio personnel in Northern Nigeria are used in increasing access to zero-dose OPV, RI, and selected PHC services. The increase in the services generated represented the increasing role of the dedicated mobile teams and polio VCMs in strengthening RI.
尼日利亚的脊髓灰质炎根除倡议始于20多年前,面临诸多挑战,包括最初的否认、社区的抵制以及长期的地区安全担忧。这些挑战促使制定应对措施,包括制定国家应急行动计划、改善合作伙伴协调和政府参与,以及设立脊髓灰质炎应急行动中心。尽管每月的补充免疫活动(SIAs)仍在继续,但利用专门的流动团队和志愿社区动员者(VCMs),针对脊髓灰质炎传播高风险定居点开展常规免疫(RI)和其他选定的初级卫生保健(PHC)服务,成为在高风险地区阻断脊髓灰质炎传播的关键策略。这些努力可能促成了2014年7月24日至2016年8月11日期间连续两年无野生脊髓灰质炎病毒,不过之后尼日利亚北部博尔诺州报告了2例该病毒病例。
对与脊髓灰质炎相关的项目及其他官方文件进行叙述性分析,以确定相关人力资源及其在脊髓灰质炎根除倡议和常规免疫中的作用。本文使用的数据来自联合国儿童基金会(UNICEF)和世界卫生组织的项目报告,以及尼日利亚北部专门流动团队方法的一份评估报告草稿。
2014年开始采用专门流动团队方法提供脊髓灰质炎、常规免疫和其他选定初级卫生保健服务的6个州的数据显示,脊髓灰质炎传播高风险定居点中持有常规免疫卡的12至23个月儿童的比例总体从23%增至56%,12至23个月完全免疫儿童的比例总体从19%增至55%。2013年至2015年期间,按照常规免疫时间表接种第一剂口服脊髓灰质炎疫苗(OPV)的新生儿数量以及在志愿社区动员者协助下接种零剂OPV的儿童数量同样有所增加。2015年,志愿社区动员者在这6个州帮助追踪了167,092名新生儿,并使156,537名1岁以下婴儿获得常规免疫服务。
分析表明,尼日利亚北部的脊髓灰质炎防治人员在增加零剂OPV、常规免疫和选定的初级卫生保健服务可及性方面发挥了作用。所提供服务的增加体现了专门流动团队和脊髓灰质炎志愿社区动员者在加强常规免疫方面日益重要的作用。