Environmental and Autonomic Physiology Laboratory, Department of Kinesiology and Health Education, The University of Texas at Austin, Austin, TX, United States.
Environmental and Autonomic Physiology Laboratory, Department of Kinesiology and Health Education, The University of Texas at Austin, Austin, TX, United States; Integrative Vascular Physiology Laboratory, Department of Kinesiology, The University of Texas at Arlington, Arlington, TX, United States.
Microvasc Res. 2018 Jan;115:52-57. doi: 10.1016/j.mvr.2017.08.005. Epub 2017 Aug 24.
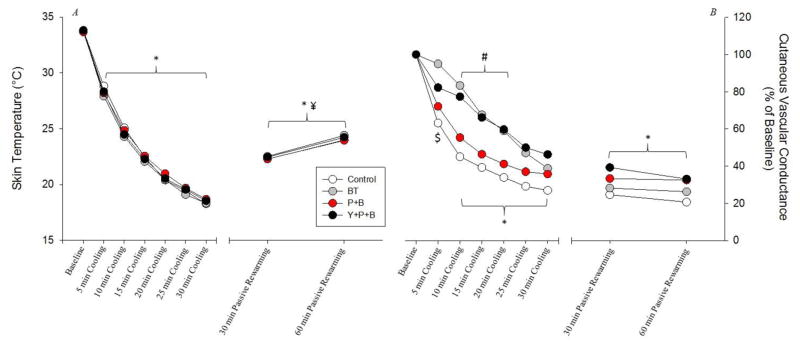
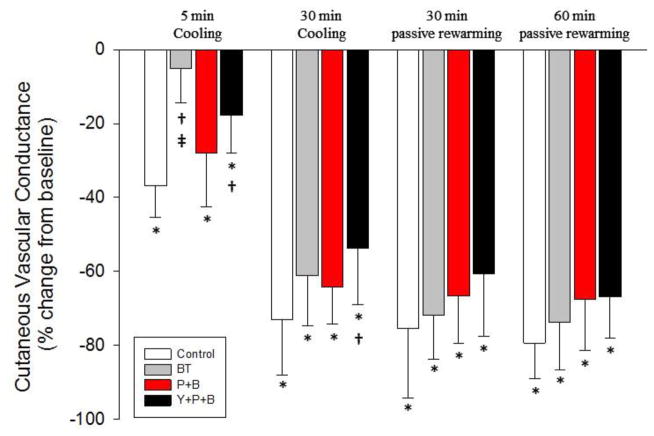
Cryotherapy is a therapeutic technique using ice or cold water applied to the skin to manage soft tissue trauma and injury. While beneficial, there are some potentially detrimental side effects, such as pronounced vasoconstriction and tissue ischemia that are sustained for hours post-treatment. This study tested the hypothesis that this vasoconstriction is mediated by 1) activation of post-synaptic α-adrenergic receptors and/or 2) activation of post-synaptic neuropeptide Y1 (NPY Y1) receptors. 8 subjects were fitted with a commercially available cryotherapy unit with a water perfused bladder on the lateral portion of the right calf. Participants were instrumented with four intradermal microdialysis probes beneath the bladder. The following conditions were applied at the four treatment sites: 1) control (Ringer solution), 2) combined post-synaptic β-adrenergic receptors and neuropeptide (NPY) Y receptors blockade (P+B site), 3) combined post-synaptic α-adrenergic receptor, β-adrenergic receptor, and NPY Y receptor blockade (Y+P+B site), and 4) blockade of pre-synaptic release of all neurotransmitters from the sympathetic nerves (BT site). Following thermoneutral baseline data collection, 1°C water was perfused through the bladder for 30min, followed by passive rewarming for 60min. Skin temperature (T) fell from ~34°C to ~18.5°C during active cooling across all sites and there was no difference between sites (P>0.05 vs. control for each site). During passive rewarming T rose to a similar degree in all sites (P>0.05 relative to the end of cooling). In the first 20min of cooling %CVC was reduced at all sites however, this response was blunted in the BT and the Y+P+B sites (P>0.05 for all comparisons). By the end of cooling the degree of vasoconstriction was similar between sites with the exception that the reduction in %CVC in the Y+B+P site was less relative to the reduction in the control site. %CVC was unchanged in any of the sites during passive rewarming such that each remained similar to values obtained at the end of active cooling. These findings indicate that the initial vasoconstriction (i.e. within the 1st 20min) that occurs during cryotherapy induced local cooling is achieved via activation of post-synaptic α-adrenergic receptors; whereas nonadrenergic mechanisms predominate as the duration of cooling continues. The sustained vasoconstriction that occurs following cessation of the cooling stimulus does not appear to be related to activation of post-synaptic α-adrenergic receptors or NPY Y1 receptor.
冷冻疗法是一种利用冰或冷水应用于皮肤来治疗软组织创伤和损伤的治疗技术。虽然有益,但也有一些潜在的有害副作用,如治疗后数小时内持续的明显血管收缩和组织缺血。本研究测试了以下假设:这种血管收缩是由 1)突触后α-肾上腺素能受体的激活和/或 2)突触后神经肽 Y1(NPY Y1)受体的激活介导的。8 名受试者在右侧小腿外侧安装了带有水灌注膀胱的商业冷冻治疗装置。参与者在膀胱下方安装了四个皮内微透析探针。在四个治疗部位施加以下条件:1)对照(林格氏溶液),2)联合突触后β-肾上腺素能和神经肽(NPY)Y 受体阻断(P+B 部位),3)联合突触后α-肾上腺素能受体、β-肾上腺素能受体和 NPY Y 受体阻断(Y+P+B 部位),以及 4)阻断来自交感神经的所有神经递质的节前释放(BT 部位)。在收集到温热基线数据后,将 1°C 的水通过膀胱灌注 30 分钟,然后进行 60 分钟的被动复温。在所有部位,皮肤温度(T)从34°C 降至18.5°C,且各部位之间无差异(与各部位的对照相比,P>0.05)。在被动复温过程中,T 在所有部位上升到相似的程度(与冷却结束时相比,P>0.05)。在冷却的前 20 分钟,所有部位的%CVC 均降低,但 BT 和 Y+P+B 部位的反应减弱(与所有比较相比,P>0.05)。到冷却结束时,除了 Y+B+P 部位的%CVC 减少幅度小于对照部位外,各部位的血管收缩程度相似。在被动复温期间,任何部位的%CVC 均未发生变化,因此每个部位均与主动冷却结束时获得的值相似。这些发现表明,冷冻疗法诱导局部冷却时发生的初始血管收缩(即在第 1 至 20 分钟内)是通过激活突触后α-肾上腺素能受体实现的;而随着冷却时间的延长,非肾上腺素能机制占主导地位。在冷却刺激停止后发生的持续血管收缩似乎与突触后α-肾上腺素能受体或 NPY Y1 受体的激活无关。