Curtis Elana, Wikaire Erena, Jiang Yannan, McMillan Louise, Loto Robert, Poole Phillippa, Barrow Mark, Bagg Warwick, Reid Papaarangi
Te Kupenga Hauora Māori, Faculty of Medical and Health Sciences, University of Auckland, Auckland, New Zealand.
Department of Statistics, Faculty of Science, University of Auckland, Auckland, New Zealand.
BMJ Open. 2017 Aug 27;7(8):e017276. doi: 10.1136/bmjopen-2017-017276.
To determine associations between admission markers of socioeconomic status, transitioning, bridging programme attendance and prior academic preparation on academic outcomes for indigenous Māori, Pacific and rural students admitted into medicine under access pathways designed to widen participation. Findings were compared with students admitted via the general (usual) admission pathway.
Retrospective observational study using secondary data.
6-year medical programme (MBChB), University of Auckland, Aotearoa New Zealand. Students are selected and admitted into Year 2 following a first year (undergraduate) or prior degree (graduate).
1676 domestic students admitted into Year 2 between 2002 and 2012 via three pathways: GENERAL admission (1167), Māori and Pacific Admission Scheme-MAPAS (317) or Rural Origin Medical Preferential Entry-ROMPE (192). Of these, 1082 students completed the programme in the study period.
Graduated from medical programme (yes/no), academic scores in Years 2-3 (Grade Point Average (GPA), scored 0-9).
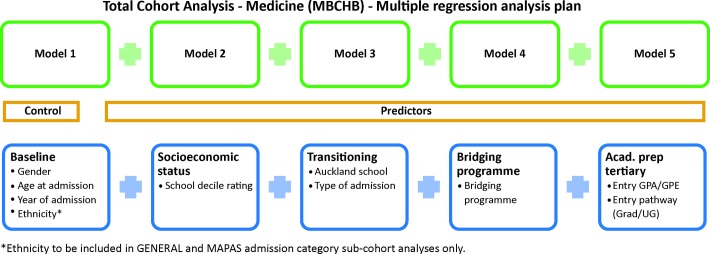
735/778 (95%) of GENERAL, 111/121 (92%) of ROMPE and 146/183 (80%) of MAPAS students graduated from intended programme. The graduation rate was significantly lower in the MAPAS students (p<0.0001). The average Year 2-3 GPA was 6.35 (SD 1.52) for GENERAL, which was higher than 5.82 (SD 1.65, p=0.0013) for ROMPE and 4.33 (SD 1.56, p<0.0001) for MAPAS. Multiple regression analyses identified three key predictors of better academic outcomes: bridging programme attendance, admission as an undergraduate and admission GPA/Grade Point Equivalent (GPE). Attending local urban schools and higher school deciles were also associated with a greater likelihood of graduation. All regression models have controlled for predefined baseline confounders (gender, age and year of admission).
There were varied associations between admission variables and academic outcomes across the three admission pathways. Equity-targeted admission programmes inclusive of variations in academic threshold for entry may support a widening participation agenda, however, additional academic and pastoral supports are recommended.
确定社会经济地位、过渡情况、衔接课程参与度及先前学业准备等入学指标与通过旨在扩大参与度的入学途径进入医学专业的毛利族、太平洋岛民和农村学生学业成绩之间的关联。将研究结果与通过普通(常规)入学途径录取的学生进行比较。
利用二手数据进行的回顾性观察研究。
新西兰奥塔哥大学为期6年的医学课程(MBChB)。学生在完成第一年(本科)或先前学位(研究生)学习后被选拔进入二年级。
2002年至2012年间通过三种途径进入二年级的1676名国内学生:普通入学(1167人)、毛利族和太平洋岛民入学计划-MAPAS(317人)或农村生源医学优先入学-ROMPE(192人)。其中,1082名学生在研究期间完成了该课程。
从医学课程毕业(是/否),2至3年级的学业成绩(平均绩点(GPA),评分0至9)。
普通入学途径的学生中有735/778(95%)、ROMPE途径的学生中有111/121(92%)、MAPAS途径的学生中有146/183(80%)从预期课程毕业。MAPAS途径的学生毕业率显著较低(p<0.0001)。普通入学途径学生2至3年级的平均GPA为6.35(标准差1.52),高于ROMPE途径的5.82(标准差1.65,p=0.0013)和MAPAS途径的4.33(标准差1.56,p<0.0001)。多元回归分析确定了学业成绩较好的三个关键预测因素:参加衔接课程、本科入学以及入学GPA/同等绩点(GPE)。就读当地城市学校和学校排名较高也与毕业可能性较大相关。所有回归模型均对预先定义的基线混杂因素(性别、年龄和入学年份)进行了控制。
三种入学途径的入学变量与学业成绩之间存在不同的关联。包括入学学术门槛差异在内的公平性入学计划可能有助于推动扩大参与度议程,然而,建议提供额外的学术和辅导支持。