Spero Kerry, Bayasi Ghiath, Beaudry Linda, Barber Kimberly R, Khorfan Fahim
Department of Medical Education, Genesys Regional Medical Center, Grand Blanc.
Department of Pulmonary and Critical Care Medicine, Michigan State University, East Lansing.
Int J Chron Obstruct Pulmon Dis. 2017 Aug 11;12:2417-2423. doi: 10.2147/COPD.S139919. eCollection 2017.
The diagnosis of chronic obstructive pulmonary disease (COPD) is usually made based on history and physical exam alone. Symptoms of dyspnea, cough, and wheeze are nonspecific and attributable to a variety of diseases. Confirmatory testing to verify the airflow obstruction is available but rarely used, which may result in substantial misdiagnoses of COPD. The aim of this study is to evaluate the use of confirmatory testing and assess the accuracy of the diagnosis.
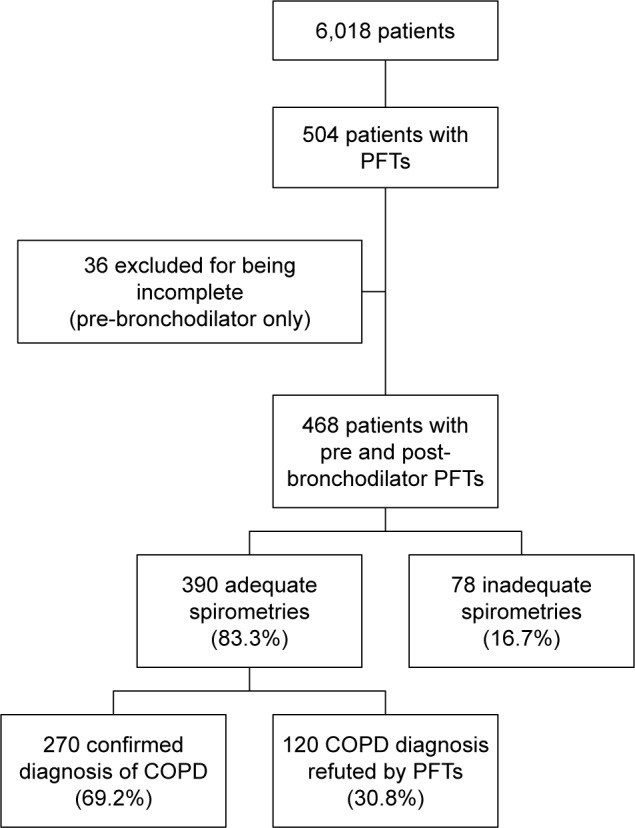
From January 2011 through December 2013, 6,018 patients with COPD as a principal or leading diagnosis were admitted at a community teaching hospital. Of those, only 504 (8.4%) patients had spirometry performed during hospitalization. The studies were reviewed by two board-certified pulmonologists to verify presence of persistent airflow obstruction. Charts of these patients were then examined to determine if the spirometry results had changed the diagnosis or the treatment plan for these patients.
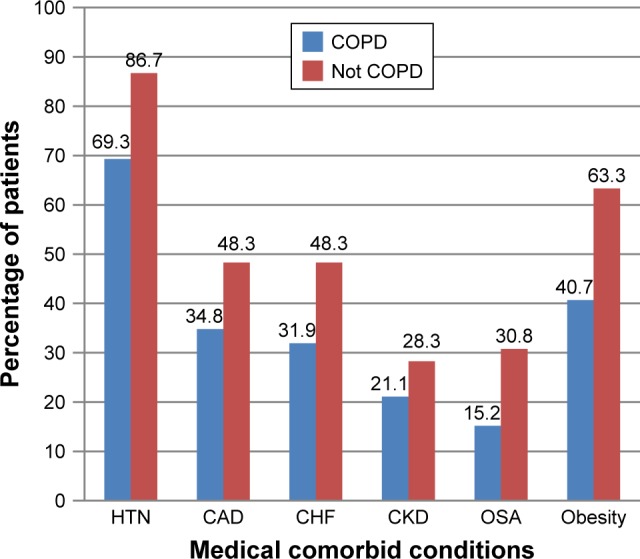
Spirometry confirmed the diagnosis of COPD in 270 patients (69.2%) treated as COPD during their hospitalization. Restrictive lung disease was found to be present in 104 patients (26.6%) and normal in 16 patients (4.2%). Factors predictive of airflow obstruction included smoking status and higher pack-year history. Negative predictive factors included higher body mass index (BMI) and other medical comorbidities. These patients were significantly more likely to be misdiagnosed and mistreated as COPD.
Up to a third of patients diagnosed and treated as COPD in the hospital may be inaccurately diagnosed as COPD based on confirmatory spirometry testing. Factors contributing to the inaccuracy of diagnosis include less smoking history, high BMI, and associated comorbidities.
慢性阻塞性肺疾病(COPD)的诊断通常仅基于病史和体格检查。呼吸困难、咳嗽和喘息症状并无特异性,可归因于多种疾病。虽然有用于验证气流受限的确诊检测方法,但很少使用,这可能导致COPD的大量误诊。本研究的目的是评估确诊检测的使用情况并评估诊断的准确性。
2011年1月至2013年12月期间,一家社区教学医院收治了6018例以COPD作为主要或首要诊断的患者。其中,只有504例(8.4%)患者在住院期间进行了肺功能测定。两位获得委员会认证的肺科医生对这些研究进行了审查,以确认是否存在持续性气流受限。然后检查这些患者的病历,以确定肺功能测定结果是否改变了这些患者的诊断或治疗方案。
肺功能测定确诊了270例(69.2%)住院期间被诊断为COPD的患者。发现104例(26.6%)患者存在限制性肺病,16例(4.2%)患者肺功能正常。气流受限的预测因素包括吸烟状况和更高的吸烟包年史。负性预测因素包括更高的体重指数(BMI)和其他合并症。这些患者被误诊和误治为COPD的可能性显著更高。
根据确诊的肺功能测定结果,在医院被诊断和治疗为COPD的患者中,高达三分之一可能被不准确地诊断为COPD。导致诊断不准确的因素包括吸烟史较少、BMI较高和相关合并症。