Department of Medicine, Section of Geriatrics and Palliative Medicine, The University of Chicago, Chicago, IL.
University at Buffalo School of Medicine, Buffalo, NY.
J Am Med Dir Assoc. 2017 Dec 1;18(12):1082-1086. doi: 10.1016/j.jamda.2017.07.005. Epub 2017 Aug 31.
There are limited screening tools to predict adverse postoperative outcomes for the geriatric surgical fracture population. Frailty is increasingly recognized as a risk assessment to capture complexity. The goal of this study was to use a short screening tool, the FRAIL scale, to categorize the level of frailty of older adults admitted with a fracture to determine the association of each frailty category with postoperative and 30-day outcomes.
Retrospective cohort study.
Level 1 trauma center.
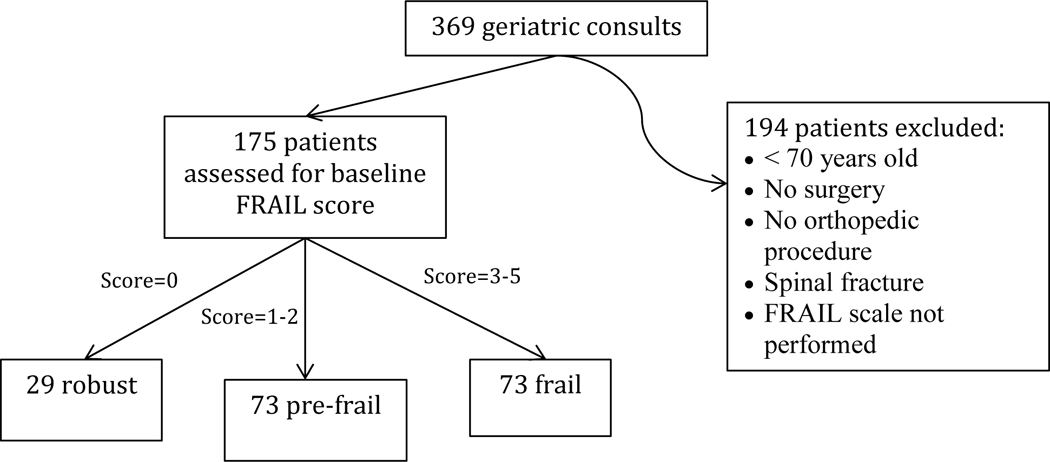
A total of 175 consecutive patients over age 70 years admitted to co-managed orthopedic trauma and geriatrics services.
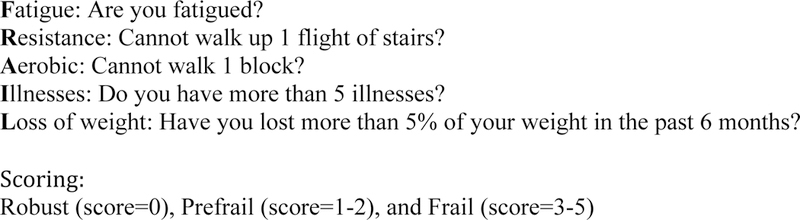
The FRAIL scale (short 5-question assessment of fatigue, resistance, aerobic capacity, illnesses, and loss of weight) classified the patients into 3 categories: robust (score = 0), prefrail (score = 1-2), and frail (score = 3-5). Postoperative outcome variables collected were postoperative complications, unplanned intensive care unit admission, length of stay (LOS), discharge disposition, and orthopedic follow-up after surgery. Thirty-day outcomes measured were 30-day readmission and 30-day mortality. Analysis of variance (1-way) and Kruskal-Wallis tests were used to compare continuous variables across the 3 FRAIL categories. Fisher exact tests were used to compare categorical variables. Multiple regression analysis, adjusted by age, sex, and Charlson index, was conducted to study the association between frailty category and outcomes.
FRAIL scale categorized the patients into 3 groups: robust (n = 29), prefrail (n = 73), and frail (n = 73). There were statistically significant differences between groups in terms of age, comorbidity, dementia, functional dependency, polypharmacy, and rate of institutionalization, being higher in the frailest patients. Hip fracture was the most frequent fracture, and it was more frequent as the frailty of the patient increased (48%, 61%, and 75% in robust, prefrail, and frail groups, respectively). The American Society of Anesthesiologists preoperative risk significantly correlated with the frailty of the patient (American Society of Anesthesiologists score 3-4: 41%, 82% and 86%, in robust, prefrail, and frail groups, P < .001). After adjustment by age, sex, and comorbidity, there was a statistically significant association between frailty and both LOS and the development of any complication after surgery (LOS: 4.2, 5.0, and 7.1 days, P = .002; any complication: 3.4%, 26%, and 39.7%, P = .03; in robust, prefrail, and frail groups). There were also significant differences in discharge disposition (31% of robust vs 4.1% frail, P = .008) and follow-up completion (97% of robust vs 69% of the frail ones). Differences in time to surgery, unplanned intensive care unit admission, and 30-day readmission and mortality, although showing a trend, did not reach statistical significance.
Frailty, measured by the FRAIL scale, was associated with increase LOS, complications after surgery, and discharge to rehabilitation facility in geriatric fracture patients. The FRAIL scale is a promising short screen to stratify and help operationalize the perioperative care of older surgical patients.
针对老年外科骨折患者,目前用于预测不良术后结果的筛选工具十分有限。虚弱越来越被认为是一种评估风险的手段,以捕捉复杂性。本研究的目的是使用一种简短的筛选工具(FRAIL 量表)对患有骨折的老年人进行虚弱程度分类,以确定每个虚弱类别与术后和 30 天结果的关联。
回顾性队列研究。
1 级创伤中心。
共纳入 175 名连续年龄在 70 岁以上的患者,这些患者在骨科创伤和老年科联合管理下入院。
FRAIL 量表(疲劳、抵抗力、有氧运动能力、疾病和体重减轻的简短 5 项评估)将患者分为 3 类:强壮(评分=0)、虚弱前期(评分=1-2)和虚弱(评分=3-5)。收集的术后结果变量包括术后并发症、非计划转入重症监护病房、住院时间(LOS)、出院去向和术后骨科随访。30 天结果测量为 30 天再入院和 30 天死亡率。方差分析(1 -way)和 Kruskal-Wallis 检验用于比较 3 个 FRAIL 类别之间的连续变量。Fisher 确切检验用于比较分类变量。采用多元回归分析,调整年龄、性别和 Charlson 指数,研究虚弱类别与结局之间的关系。
FRAIL 量表将患者分为 3 组:强壮(n=29)、虚弱前期(n=73)和虚弱(n=73)。各组之间在年龄、合并症、痴呆、功能依赖性、多药治疗和机构化率方面存在统计学差异,最虚弱的患者的这些差异最高。髋部骨折是最常见的骨折,随着患者的虚弱程度增加,骨折的发生率也随之增加(强壮、虚弱前期和虚弱组分别为 48%、61%和 75%)。美国麻醉师协会术前风险与患者的虚弱程度显著相关(美国麻醉师协会评分 3-4:在强壮、虚弱前期和虚弱组中分别为 41%、82%和 86%,P<.001)。在调整年龄、性别和合并症后,虚弱与 LOS 和术后任何并发症的发生均存在统计学关联(LOS:4.2、5.0 和 7.1 天,P=.002;任何并发症:3.4%、26%和 39.7%,P=.03;在强壮、虚弱前期和虚弱组)。出院去向(强壮组 31% vs 虚弱组 4.1%,P=.008)和完成随访(强壮组 97% vs 虚弱组 69%,P=.008)也存在显著差异。尽管手术时间、非计划转入重症监护病房和 30 天再入院和死亡率存在差异,但未达到统计学意义。
用 FRAIL 量表测量的虚弱与老年骨折患者的 LOS 延长、术后并发症以及康复机构出院有关。FRAIL 量表是一种有前途的短期筛查工具,可以对老年手术患者进行分层,并有助于围手术期护理。