Kelm Anna, Sollmann Nico, Ille Sebastian, Meyer Bernhard, Ringel Florian, Krieg Sandro M
Department of Neurosurgery, Klinikum rechts der Isar, Technische Universität München, Munich, Germany.
TUM-Neuroimaging Center, Klinikum rechts der Isar, Technische Universität München, Munich, Germany.
Front Oncol. 2017 Aug 18;7:176. doi: 10.3389/fonc.2017.00176. eCollection 2017.
During awake craniotomy for tumor resection, a neuropsychologist (NP) is regarded as a highly valuable partner for neurosurgeons. However, some centers do not routinely involve an NP, and data to support the high influence of the NP on the perioperative course of patients are mostly lacking.
The aim of this study was to investigate whether there is a difference in clinical outcomes between patients who underwent awake craniotomy with and without the attendance of an NP.
Our analysis included 61 patients, all operated on for resection of a presumably language-eloquent glioma during an awake procedure. Of these 61 cases, 47 surgeries were done with neuropsychological support (NP group), whereas 14 surgeries were performed without an NP (non-NP group) due to a language barrier between the NP and the patient. For these patients, neuropsychological assessment was provided by a bilingual resident.
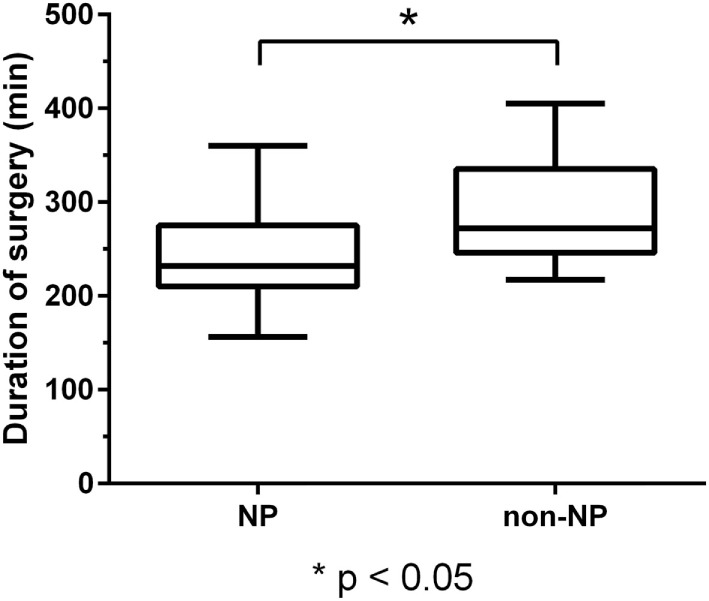
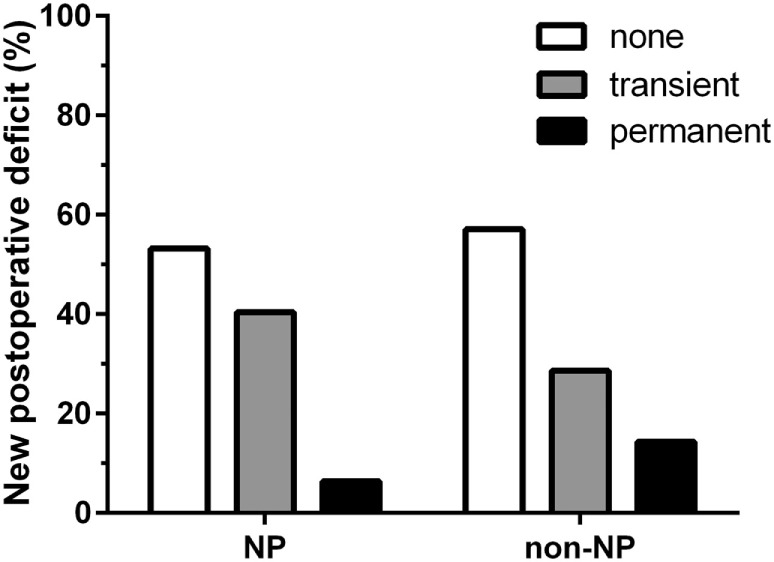
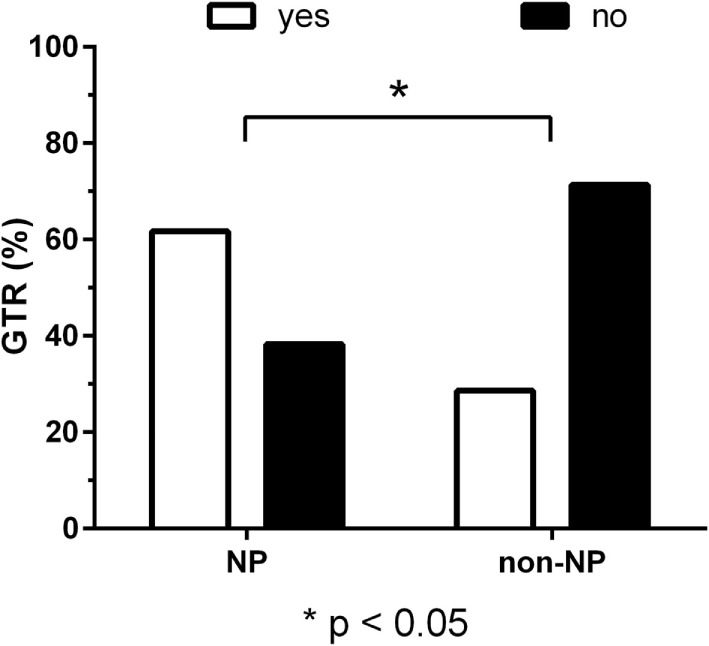
Both groups were highly comparable regarding age, gender, preoperative language function, and tumor grades (glioma WHO grades 1-4). Gross total resection (GTR) was achieved more frequently in the NP group (NP vs. non-NP: 61.7 vs. 28.6%, = 0.04), which also had shorter durations of surgery (NP vs. non-NP: 240.7 ± 45.7 vs. 286.6 ± 54.8 min, < 0.01). Furthermore, the rate of unexpected tumor residuals (estimation of the intraoperative extent of resection vs. postoperative imaging) was lower in the NP group (NP vs. non-NP: 19.1 vs. 42.9%, = 0.09), but no difference was observed in terms of permanent surgery-related language deterioration (NP vs. non-NP: 6.4 vs. 14.3%, = 0.48).
We need professional neuropsychological evaluation during awake craniotomies for removal of presumably language-eloquent gliomas. Although these procedures are routinely carried out with an NP, this is one of the first studies to provide data supporting the NP's crucial role. Despite the small group size, our study shows statistically significant results, with higher rates of GTR and shorter durations of surgery among patients of the NP group. Moreover, our data emphasize the common problem of language barriers between the surgical and neuropsychological team and patients requiring awake tumor resection.
在清醒开颅肿瘤切除术中,神经心理学家(NP)被视为神经外科医生非常有价值的合作伙伴。然而,一些中心并不常规配备NP,且大多缺乏支持NP对患者围手术期过程有重大影响的数据。
本研究旨在调查在有NP参与和无NP参与的情况下进行清醒开颅手术的患者临床结局是否存在差异。
我们的分析纳入了61例患者,均在清醒手术中接受了可能涉及语言功能区的胶质瘤切除术。在这61例病例中,47例手术有神经心理学支持(NP组),而另外14例手术因NP与患者之间存在语言障碍而未配备NP(非NP组)。对于这些患者,由一名双语住院医生进行神经心理学评估。
两组在年龄、性别、术前语言功能和肿瘤分级(世界卫生组织1-4级胶质瘤)方面具有高度可比性。NP组更常实现全切除(GTR)(NP组与非NP组:61.7%对28.6%,P = 0.04),手术时间也更短(NP组与非NP组:240.7±45.7分钟对286.6±54.8分钟,P < 0.01)。此外,NP组意外肿瘤残留率(术中切除范围估计与术后影像学检查结果对比)较低(NP组与非NP组:19.1%对42.9%,P = 0.09),但在永久性手术相关语言功能恶化方面未观察到差异(NP组与非NP组:6.4%对14.3%,P = 0.48)。
在切除可能涉及语言功能区的胶质瘤的清醒开颅手术中,我们需要专业的神经心理学评估。尽管这些手术通常由NP进行,但这是首批提供数据支持NP关键作用的研究之一。尽管样本量较小,我们的研究显示出具有统计学意义的结果,NP组患者的GTR率更高且手术时间更短。此外,我们的数据强调了手术团队和神经心理学团队与需要清醒肿瘤切除的患者之间存在语言障碍这一常见问题。