Kahler Zachary P, Musey Paul I, Schaffer Jason T, Johnson Annelyssa N, Strachan Christian C, Shufflebarger Charles M
Indiana University School of Medicine, Department of Emergency Medicine, Indianapolis, Indiana.
University of South Carolina, Greenville School of Medicine, Department of Emergency Medicine, Greenville, South Carolina.
West J Emerg Med. 2017 Aug;18(5):894-902. doi: 10.5811/westjem.2017.6.33414. Epub 2017 Jul 25.
The U.S. opioid epidemic has highlighted the need to identify patients at risk of opioid abuse and overdose. We initiated a novel emergency department- (ED) based interventional protocol to transition our superuser patients from the ED to an outpatient chronic pain program. The objective was to evaluate the protocol's effect on superusers' annual ED visits. Secondary outcomes included a quantitative evaluation of statewide opioid prescriptions for these patients, unique prescribers of controlled substances, and ancillary testing.
Patients were referred to the program with the following inclusion criteria: ≥ 6 visits per year to the ED; at least one visit identified by the attending physician as primarily driven by opioid-seeking behavior; and a review by a committee comprising ED administration and case management. Patients were referred to a pain management clinic and informed that they would no longer receive opioid prescriptions from visits to the ED for chronic pain complaints. Electronic medical record (EMR) alerts notified ED providers of the patient's referral at subsequent visits. We analyzed one year of data pre- and post-referral.
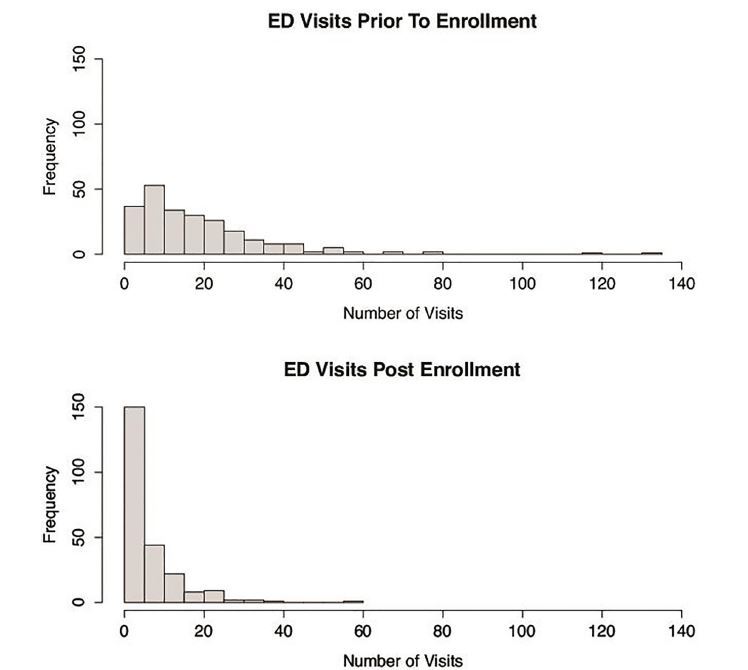
A total of 243 patients had one year of data post-referral for analysis. Median annual ED visits decreased from 14 to 4 (58% decrease, 95% CI [50 to 66]). We also found statistically significant decreases for these patients' state prescription drug monitoring program (PDMP) opioid prescriptions (21 to 13), total unique controlled-substance prescribers (11 to 7), computed tomography imaging (2 to 0), radiographs (5 to 1), electrocardiograms (12 to 4), and labs run (47 to 13).
This program and the EMR-based alerts were successful at decreasing local ED visits, annual opioid prescriptions, and hospital resource allocation for this population of patients. There is no evidence that these patients diverted their visits to neighboring EDs after being informed that they would not receive opioids at this hospital, as opioid prescriptions obtained by these patients decreased on a statewide level. This implies that individual ED protocols can have significant impact on the behavior of patients.
美国的阿片类药物泛滥凸显了识别有阿片类药物滥用和过量风险患者的必要性。我们启动了一项基于急诊科(ED)的新型干预方案,将我们的超级用户患者从急诊科过渡到门诊慢性疼痛项目。目的是评估该方案对超级用户年度急诊科就诊次数的影响。次要结果包括对这些患者的全州阿片类药物处方、受控物质的独特开方者以及辅助检查进行定量评估。
符合以下纳入标准的患者被转介到该项目:每年到急诊科就诊≥6次;至少有一次就诊被主治医师确定主要由寻求阿片类药物行为驱动;并由急诊科管理部门和病例管理部门组成的委员会进行审查。患者被转介到疼痛管理诊所,并被告知他们将不再因慢性疼痛投诉到急诊科就诊而获得阿片类药物处方。电子病历(EMR)警报在患者后续就诊时通知急诊科工作人员其转介情况。我们分析了转介前后一年的数据。
共有243名患者在转介后有一年的数据可供分析。年度急诊科就诊中位数从14次降至4次(减少58%,95%置信区间[50%至66%])。我们还发现这些患者的州处方药监测计划(PDMP)阿片类药物处方(从21张降至13张)、独特受控物质开方者总数(从11人降至7人)、计算机断层扫描成像(从2次降至0次)、X光片(从5次降至1次)、心电图(从12次降至4次)以及实验室检查(从47次降至13次)均有统计学意义的下降。
该项目和基于电子病历的警报成功减少了该类患者的当地急诊科就诊次数、年度阿片类药物处方以及医院资源分配。没有证据表明这些患者在被告知他们将无法在这家医院获得阿片类药物后将就诊转移到邻近的急诊科,因为这些患者获得的阿片类药物处方在全州范围内都有所减少。这意味着个别急诊科方案可能对患者行为产生重大影响。