Bello George, Faragher Brian, Sanudi Lifah, Namakhoma Ireen, Banda Hastings, Malmborg Rasmus, Thomson Rachael, Squire S Bertel
Research for Equity And Community Health (REACH) Trust, Lilongwe, Malawi.
Centre for Applied Health Research & Delivery, Liverpool School of Tropical Medicine, Pembroke Place, Liverpool, United Kingdom.
PLoS One. 2017 Sep 6;12(9):e0183312. doi: 10.1371/journal.pone.0183312. eCollection 2017.
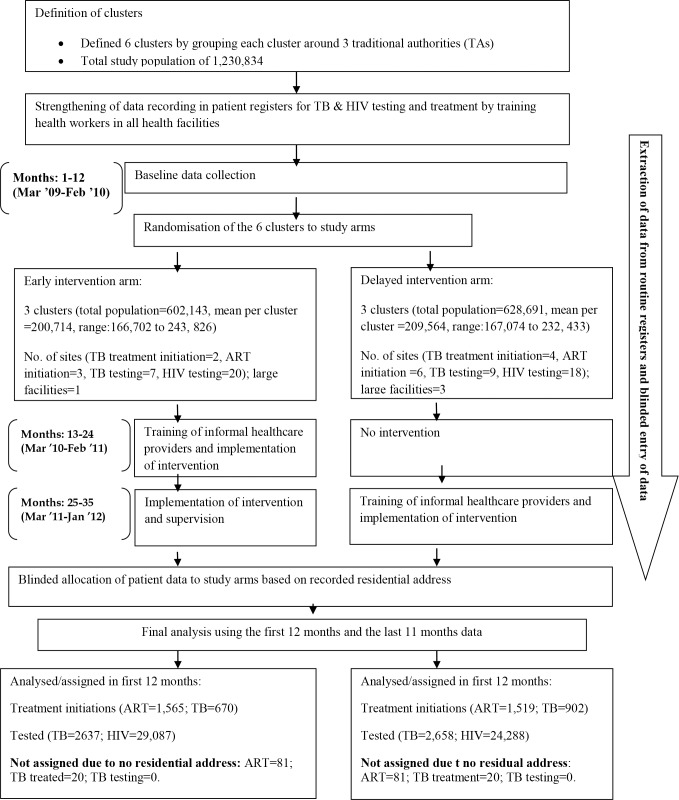
The poor face barriers in accessing services for tuberculosis (TB) and Human Immuno-deficiency Virus (HIV) disease. A cluster randomised trial was conducted to investigate the effectiveness of engaging unpaid informal providers (IPs) to promote access in a rural district. The intervention consisted of training unpaid IPs in TB and HIV disease recognition, sputum specimen collection, appropriate referrals, and raising community awareness.
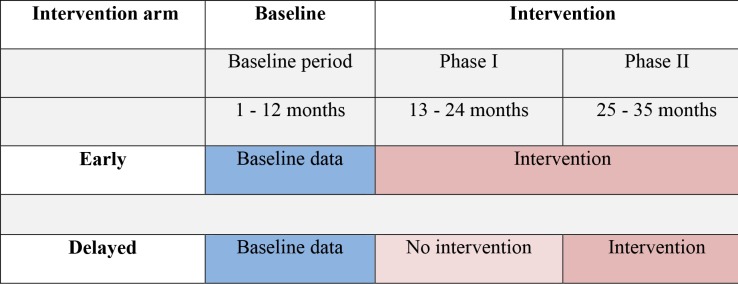
In total, six clusters were defined in the study areas. Through a pair-matched cluster randomization process, three clusters (average cluster population = 200,714) were allocated to receive the intervention in the Early arm. Eleven months later the intervention was rolled out to the remaining three clusters (average cluster population = 209,564)-the Delayed arm. Treatment initiation rates for TB and Anti-Retroviral Therapy (ART) were the primary outcome measures. Secondary outcome measures included testing rates for TB and HIV. We report the results of the comparisons between the Early and Delayed arms over the 23 month trial period. Data were obtained from patient registers. Poisson regression models with robust standard errors were used to express the effectiveness of the intervention as incidence rate ratios (IRR).
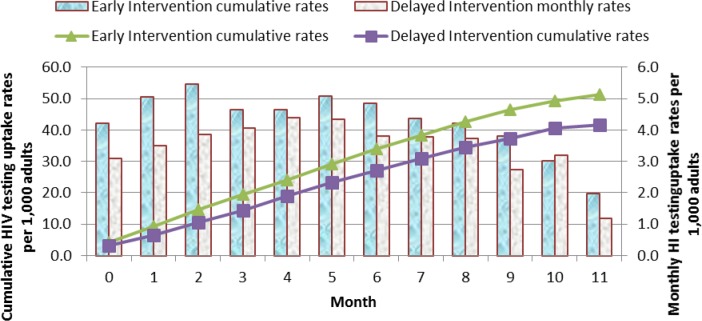
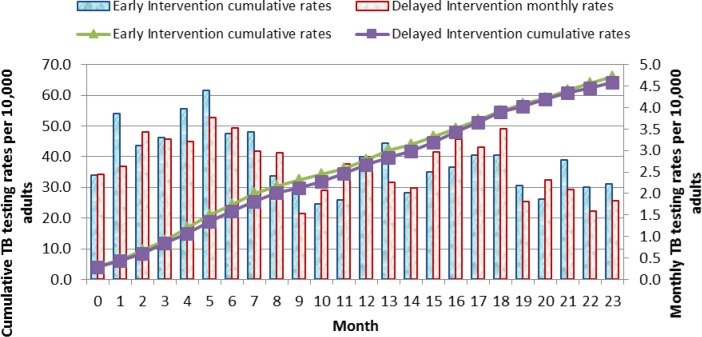
The Early and Delayed clusters were well matched in terms of baseline monthly mean counts and incidence rate ratios for TB and ART treatment initiation. However there were fewer testing and treatment initiation facilities in the Early clusters (TB treatment n = 2, TB testing n = 7, ART initiation n = 3, HIV testing n = 20) than in the Delayed clusters (TB treatment n = 4, TB testing n = 9, ART initiation n = 6, HIV testing n = 18). Overall there were more HIV testing and treatment centres than TB testing and treatment centres. The IRR was 1.18 (95% CI: 0.903-1.533; p = 0.112) for TB treatment initiation and 1.347 (CI:1.00-1.694; p = 0.049) for ART initiation in the first 12 months and the IRR were 0.552 (95% CI:0.397-0.767; p<0.001) and 0.924 (95% CI: 0.369-2.309, p = 0.863) for TB and ART treatment initiations respectively for the last 11 months. The IRR were 1.152 (95% CI:1.009-1.359, p = 0.003) and 1.61 (95% CI:1.385-1.869, p<0.001) for TB and HIV testing uptake respectively in the first 12 months. The IRR was 0.659 (95% CI:0.441-0.983; p = 0.023) for TB testing uptake for the last 11 months.
We conclude that engagement of unpaid IPs increased TB and HIV testing rates and also increased ART initiation. However, for these providers to be effective in promoting TB treatment initiation, numbers of sites offering TB testing and treatment initiation in rural areas should be increased.
ClinicalTrials.gov NCT02127983.
结核病(TB)和人类免疫缺陷病毒(HIV)疾病患者在获取服务方面面临诸多障碍。开展了一项整群随机试验,以调查让无报酬的非正式服务提供者(IPs)参与进来以促进农村地区服务可及性的有效性。干预措施包括对无报酬的IPs进行结核病和HIV疾病识别、痰标本采集、适当转诊方面的培训,以及提高社区意识。
在研究区域总共定义了6个群组。通过配对整群随机化过程,三个群组(平均群组人口 = 200,714)被分配到早期组接受干预。11个月后,干预措施推广到其余三个群组(平均群组人口 = 209,564)——延迟组。结核病治疗启动率和抗逆转录病毒疗法(ART)启动率是主要结局指标。次要结局指标包括结核病和HIV检测率。我们报告了在23个月试验期内早期组和延迟组之间比较的结果。数据从患者登记册中获取。使用具有稳健标准误的泊松回归模型将干预效果表示为发病率比(IRR)。
早期组和延迟组在结核病和ART治疗启动的基线月平均计数和发病率比方面匹配良好。然而,早期组中提供检测和治疗启动的设施(结核病治疗n = 2,结核病检测n = 7,ART启动n = 3,HIV检测n = 20)比延迟组(结核病治疗n = 4,结核病检测n = 9,ART启动n = 6,HIV检测n = 18)少。总体而言,HIV检测和治疗中心比结核病检测和治疗中心更多。前12个月结核病治疗启动的IRR为1.18(95%CI:0.903 - 1.533;p = 0.112),ART启动的IRR为1.347(CI:1.00 - 1.694;p = 0.049),后11个月结核病和ART治疗启动的IRR分别为0.552(95%CI:0.397 - 0.767;p<0.001)和0.924(95%CI:0.369 - 2.309,p = 0.863)。前12个月结核病和HIV检测接受率的IRR分别为1.152(95%CI:1.009 - 1.359,p = 0.003)和1.61(95%CI:1.385 - 1.869,p<0.001)。后11个月结核病检测接受率的IRR为0.659(95%CI:0.441 - 0.983;p = 0.023)。
我们得出结论,让无报酬的IPs参与进来提高了结核病和HIV检测率,也提高了ART启动率。然而,要使这些服务提供者有效促进结核病治疗启动,应增加农村地区提供结核病检测和治疗启动的场所数量。
ClinicalTrials.gov NCT02127983。