Clinical Group, Liverpool School of Tropical Medicine, Liverpool, Merseyside, United Kingdom.
PLoS One. 2012;7(9):e44794. doi: 10.1371/journal.pone.0044794. Epub 2012 Sep 11.
Poor rates of linkage from HIV diagnosis to ART initiation are a major barrier to universal coverage of ART in sub-Saharan Africa, with reasons for failure poorly understood. In the first study of this kind at primary care level, we investigated the pathway to care in the Malawian National Programme, one of the strongest in Africa.
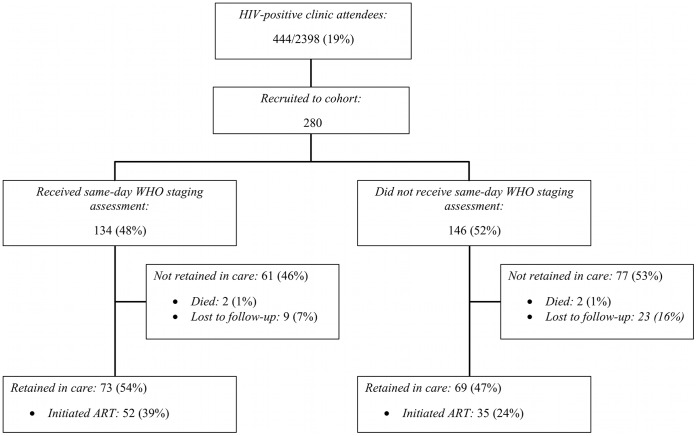
A prospective cohort study was undertaken at two primary care clinics in Blantyre, Malawi. Newly diagnosed HIV-positive adults (>15 years) were followed for 6-months to assess completion of eligibility assessments, initiation of ART and death. Two hundred and eighty participants were followed for 82.6 patient-years. ART eligibility assessments were problematic: only 134 (47.9%) received same day WHO staging and 121 (53.2%) completed assessments by 6-months. Completion of CD4 measurement (stage 1/2 only) was 81/153 (52.9%). By 6-months, 87/280 (31.1%) had initiated ART with higher uptake in participants who were ART eligible (68/91, 74.7%), and among participants who received same-day staging (52/134 [38.8%] vs. 35/146 [24.0%] p = 0.007). Non-completion of ART eligibility assessments (adjusted hazard ratio: 0.11, 95% CI: 0.06-0.21) was associated with failure to initiate ART. Retention in pre-ART care for non-ART initiators was low (55/193 [28.5%]). Of the 15 (5.4%) deaths, 11 (73.3%) occurred after ART initiation.
Although uptake of ART was high and prompt for patients with known eligibility, there was frequent failure to complete eligibility assessment and poor retention in pre-ART care. HIV care programmes should urgently evaluate the way patients are linked to ART. In particular, there is a critical need for simplified, same-day ART eligibility assessments, reduced requirements for hospital visits, and active defaulter follow-up.
艾滋病毒诊断与抗逆转录病毒治疗(ART)起始之间的衔接率低,是撒哈拉以南非洲普及 ART 治疗的主要障碍,而衔接失败的原因尚不清楚。在基层医疗层面的此类研究中,我们对马拉维国家方案进行了研究,该方案是非洲最强有力的方案之一。
在马拉维布兰太尔的两家基层医疗诊所开展了一项前瞻性队列研究。对新诊断为艾滋病毒阳性的成年人(>15 岁)进行了为期 6 个月的随访,以评估资格评估、开始接受 ART 和死亡的完成情况。280 名参与者随访了 82.6 人年。ART 资格评估存在问题:仅有 134 名(47.9%)患者在当天接受了世卫组织分期,121 名(53.2%)患者在 6 个月内完成了评估。仅完成 CD4 测量(仅 1/2 期)的有 153 名中的 81 名(52.9%)。6 个月时,280 名中的 87 名(31.1%)开始接受 ART,ART 资格符合的参与者接受 ART 的比例更高(68/91,74.7%),而在当天接受分期的参与者中(52/134 [38.8%] vs. 35/146 [24.0%],p = 0.007)。ART 资格评估未完成(调整后的风险比:0.11,95%CI:0.06-0.21)与未能开始接受 ART 相关。未开始接受 ART 的非 ART 资格符合者(193 名中的 55 名[28.5%])在接受 ART 前的护理中保留率低。15 例(5.4%)死亡中,有 11 例(73.3%)发生在开始接受 ART 之后。
尽管对于已知资格符合的患者,ART 的接受率很高且及时,但常常未能完成资格评估,而且在接受 ART 前的护理中保留率低。艾滋病毒护理方案应紧急评估将患者与 ART 衔接的方式。特别是,迫切需要简化、当天即可完成的 ART 资格评估,减少对医院就诊的要求,并积极追踪流失患者。