Yi Whitley M, Schoeppler Kelly E, Jaeger Jaclyn, Mueller Scott W, MacLaren Robert, Fish Douglas N, Kiser Tyree H
University of Colorado, Skaggs School of Pharmacy and Pharmaceutical Sciences, 12850 E Montview Blvd, Aurora, CO, 80045, USA.
Department of Pharmacy, University of Colorado Hospital, 12605 E 16th Ave, Aurora, CO, 80045, USA.
Ann Clin Microbiol Antimicrob. 2017 Sep 11;16(1):60. doi: 10.1186/s12941-017-0235-8.
Therapeutic drug monitoring (TDM) aims to minimize the clinical impact of posaconazole and voriconazole pharmacokinetic variability. However, its benefits on clinical outcomes are still being defined. Additionally, TDM data are limited for posaconazole IV and delayed-release tablet formulations among specific patient populations, including critically ill. The aim of this study was to determine the percentage of therapeutic posaconazole and voriconazole drug levels across all formulations in a real-world clinical setting and elucidate factors affecting attainment of target concentrations.
This study was a retrospective cohort study conducted at the University of Colorado Hospital between September 2006 and June 2015 that evaluated patients who received posaconazole or voriconazole TDM as part of routine care.
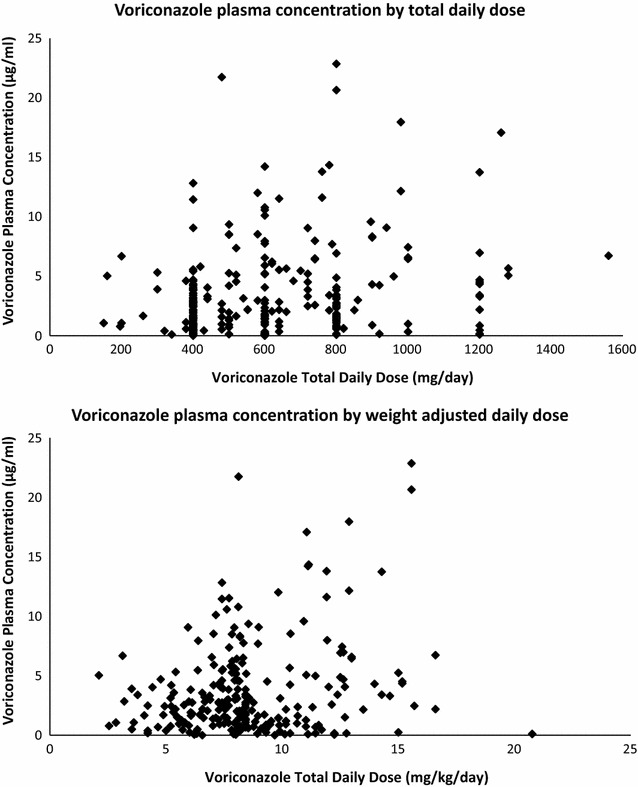
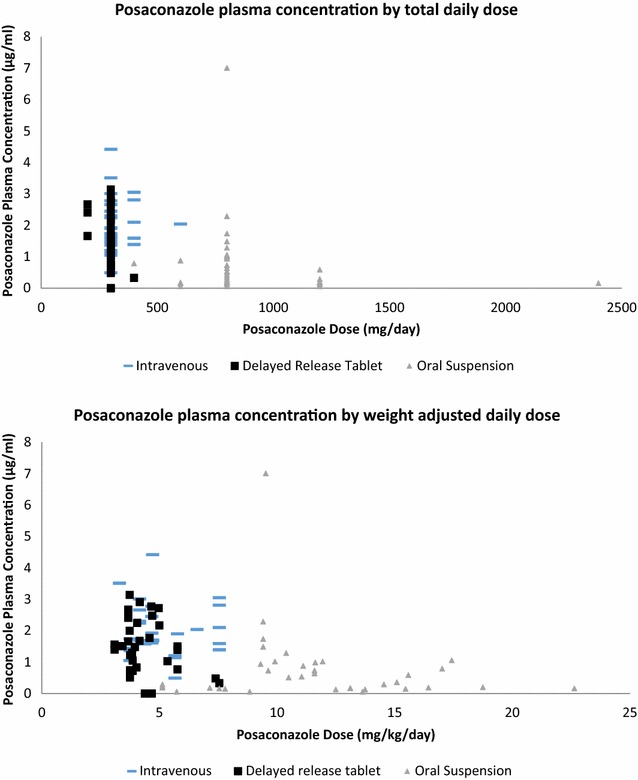
Voriconazole (n = 250) and posaconazole (n = 100) levels were analyzed from 151 patients. Of these, 54% of voriconazole and 69% of posaconazole levels were therapeutic. For posaconazole, 14/38 (37%), 28/29 (97%) and 27/33 (82%) levels were therapeutic for the oral suspension, IV, and delayed-release tablet, respectively. Intravenous and delayed-release tablet posaconazole were 20 fold (p < 0.01) and sevenfold (p = 0.002) more likely than the oral suspension to achieve a therapeutic level. Subsequent levels were more likely to be therapeutic after dose adjustments (OR 3.31; 95% CI 1.3-8.6; p = 0.02), regardless of timing of initial non-therapeutic level. In a multivariable logistic regression analysis, no characteristics were independently predictive of therapeutic voriconazole levels and only absence of H2RA/PPI use was independently predictive of therapeutic posaconazole levels. There was no correlation between survival and therapeutic drug levels for either voriconazole (p = 0.67) or posaconazole (p = 0.50).
A high percentage of drug levels did not achieve TDM targets for voriconazole and posaconazole oral suspension, supporting the need for routine TDM for those formulations. The utility of TDM for the IV and delayed-release tablet formulations of posaconazole is less apparent.
治疗药物监测(TDM)旨在将泊沙康唑和伏立康唑药代动力学变异性的临床影响降至最低。然而,其对临床结局的益处仍有待明确。此外,在包括重症患者在内的特定患者群体中,泊沙康唑静脉注射剂和缓释片剂的TDM数据有限。本研究的目的是确定在实际临床环境中所有制剂中泊沙康唑和伏立康唑达到治疗水平的百分比,并阐明影响达到目标浓度的因素。
本研究是一项回顾性队列研究,于2006年9月至2015年6月在科罗拉多大学医院进行,评估接受泊沙康唑或伏立康唑TDM作为常规治疗一部分的患者。
分析了151例患者的伏立康唑(n = 250)和泊沙康唑(n = 100)水平。其中,54%的伏立康唑水平和69%的泊沙康唑水平达到治疗标准。对于泊沙康唑,口服混悬液、静脉注射剂和缓释片剂达到治疗水平的比例分别为14/38(37%)、28/29(97%)和27/33(82%)。静脉注射用和缓释片剂泊沙康唑达到治疗水平的可能性分别比口服混悬液高20倍(p < 0.01)和7倍(p = 0.002)。剂量调整后随后的水平更有可能达到治疗标准(OR 3.31;95% CI 1.3 - 8.6;p = 0.02),无论初始未达到治疗水平的时间如何。在多变量逻辑回归分析中,没有特征能独立预测伏立康唑达到治疗水平,只有未使用H2RA/PPI能独立预测泊沙康唑达到治疗水平。伏立康唑(p = 0.67)或泊沙康唑(p = 0.50)的生存与治疗药物水平之间均无相关性。
伏立康唑和泊沙康唑口服混悬液的药物水平有很大比例未达到TDM目标,这支持了对这些制剂进行常规TDM的必要性。泊沙康唑静脉注射剂和缓释片剂的TDM效用不太明显。