Catharine Craven B, Kurban Dilnur, Farahani Farnoosh, Rivers Carly S, Ho Chester, Linassi A Gary, Gagnon Dany H, O'Connell Colleen, Ethans Karen, Bouyer Laurent J, Noonan Vanessa K
a Brain and Spinal Cord Rehabilitation Program , Toronto , ON , Canada.
b Neural Engineering & Therapeutics Team, Toronto Rehabilitation Institute , University Health Network , Toronto , ON , Canada.
J Spinal Cord Med. 2017 Nov;40(6):676-686. doi: 10.1080/10790268.2017.1368962. Epub 2017 Sep 12.
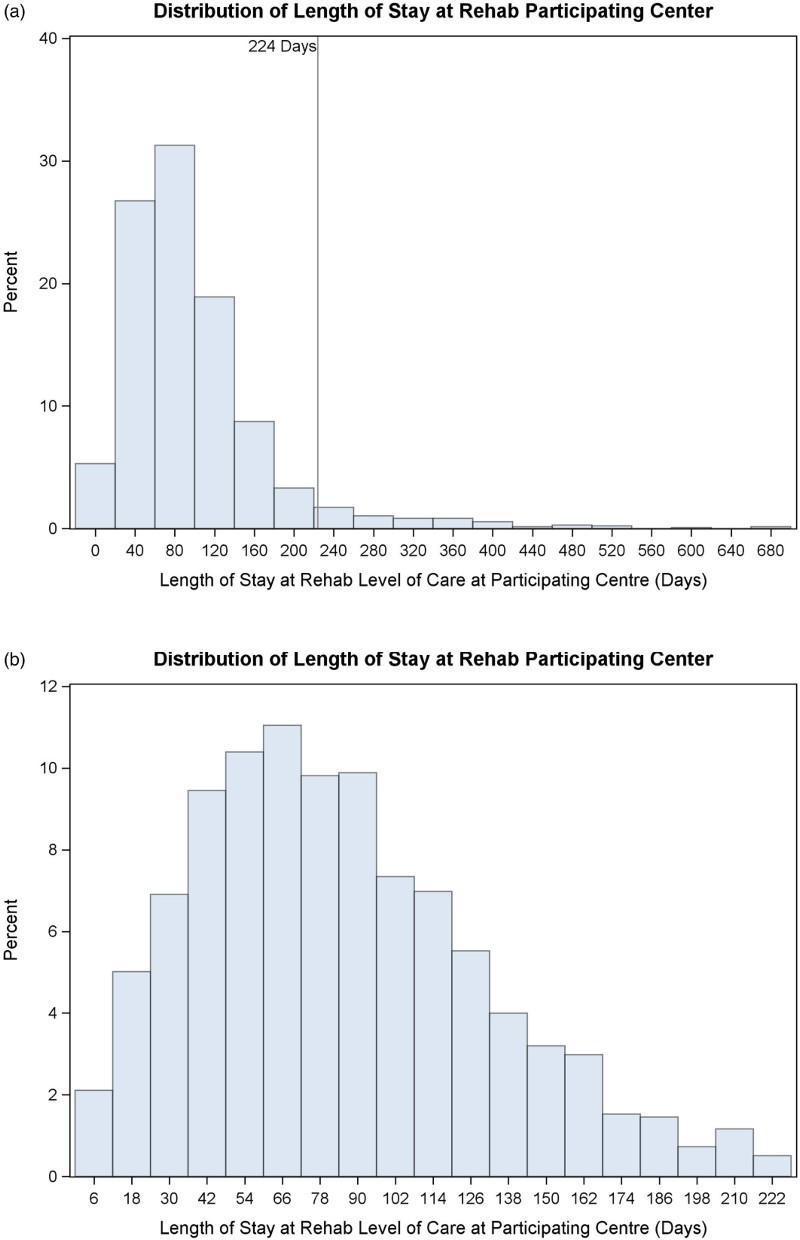
Current tertiary Spinal Cord Injury (SCI) rehabilitation funding and rehabilitation length of stay (R-LOS) in most North American jurisdictions are linked to an individual's impairment. Our objectives were to: 1) describe the impact of relevant demographic, impairment and medical complexity variables at rehabilitation admission on R-LOS among adult Canadians with traumatic SCI; and 2) identify factors which extend R-LOS.
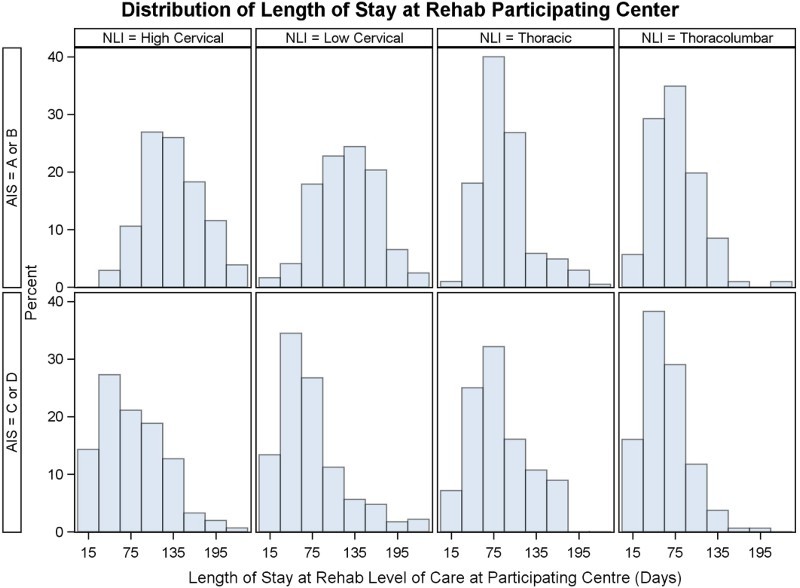
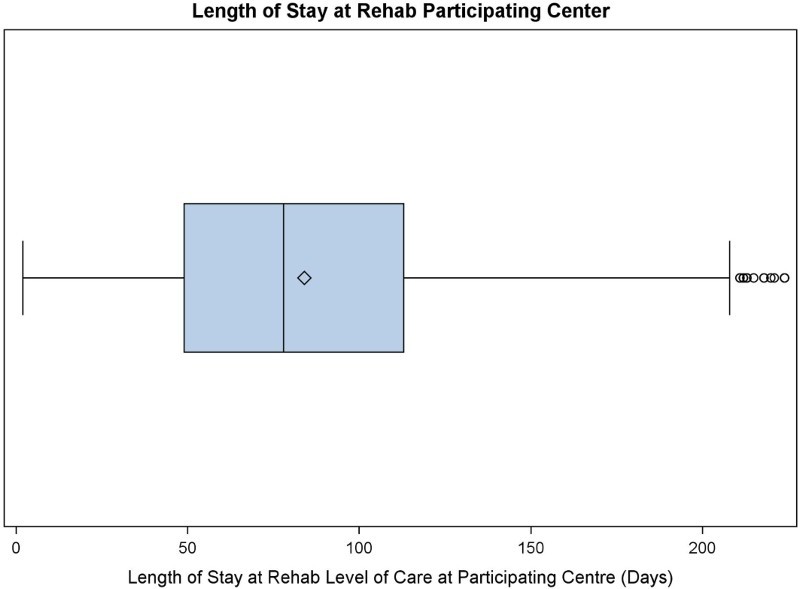
Data from 1,376 adults with traumatic SCI were obtained via chart abstraction and administrative data linkage from 15 Rick Hansen SCI Registry sites (2004-2014). Variables included age, sex, neurological impairment (level, severity), rehabilitation onset days, R-LOS, Glasgow Coma Score (GCS) at admission, prior ventilation or endotracheal tube (Vent/ETT), or indwelling bladder catheter at acute discharge, pain interference score, intensive care unit (ICU) length of stay (LOS), and lower extremity motor scores (LEMS) at rehabilitation admission. Variables related to R-LOS in bivariate analysis were included in multivariate analysis to determine their impact on R-LOS.
Prior Vent/ETT tube, indwelling bladder catheter, GCS, LEMS, and neurological impairment were related to R-LOS in bivariate analysis. Multivariate linear regression analyses identified five variables as significant predictors: age, Vent/ETT for >24 hours in acute care, indwelling bladder catheter at acute discharge, LEMS, and NLI/AIS subgroup at rehabilitation admission explained 32% of the variation in R-LOS (p<0.001).
Based on the enclosed formula, and knowledge of an individual's age at injury, spinal cord impairment (level and severity), prior Vent/ETT, presence of an indwelling bladder catheter, and LEMS at admission, administrators and clinicians may readily identify patients for whom an extended R-LOS beyond conventional LOS targets is likely.
在北美大多数司法管辖区,目前三级脊髓损伤(SCI)康复资金和康复住院时间(R-LOS)与个人损伤情况相关。我们的目标是:1)描述康复入院时相关人口统计学、损伤和医疗复杂性变量对成年创伤性SCI加拿大患者R-LOS的影响;2)确定延长R-LOS的因素。
通过图表摘要和行政数据链接,从15个里克·汉森SCI登记处(2004 - 2014年)获取了1376名成年创伤性SCI患者的数据。变量包括年龄、性别、神经损伤(水平、严重程度)、康复开始天数、R-LOS、入院时格拉斯哥昏迷评分(GCS)、急性出院时是否曾使用呼吸机或气管内插管(Vent/ETT)、或留置膀胱导管、疼痛干扰评分、重症监护病房(ICU)住院时间(LOS)以及康复入院时下肢运动评分(LEMS)。双变量分析中与R-LOS相关的变量纳入多变量分析,以确定它们对R-LOS的影响。
双变量分析中,既往Vent/ETT管、留置膀胱导管、GCS、LEMS和神经损伤与R-LOS相关。多变量线性回归分析确定了五个变量为显著预测因素:年龄、急性护理中使用Vent/ETT超过24小时、急性出院时留置膀胱导管、LEMS以及康复入院时的神经损伤程度/损伤严重程度评分(NLI/AIS)亚组解释了R-LOS变异的32%(p<0.001)。
根据所附公式,以及了解个体受伤时的年龄、脊髓损伤(水平和严重程度)、既往Vent/ETT、留置膀胱导管的存在情况以及入院时的LEMS,管理人员和临床医生可以很容易地识别出R-LOS可能超过传统LOS目标的患者。