Wang Hongyu, Dumont Xavier, Haufroid Vincent, Bernard Alfred
Louvain Centre for Toxicology and Applied Pharmacology, Institut de Recherche Expérimentale et Clinique (IREC), Université catholique de Louvain, Avenue Emmanuel Mounier 53.02, B-1200, Brussels, Belgium.
Environ Health. 2017 Sep 12;16(1):99. doi: 10.1186/s12940-017-0306-5.
Recent studies in children have reported associations of urinary cadmium (U-Cd), used as biomarker of Cd body burden, with renal dysfunction, retarded growth and impaired cognitive development in children. Little is known, however, about factors influencing U-Cd in children and likely to act as confounders.
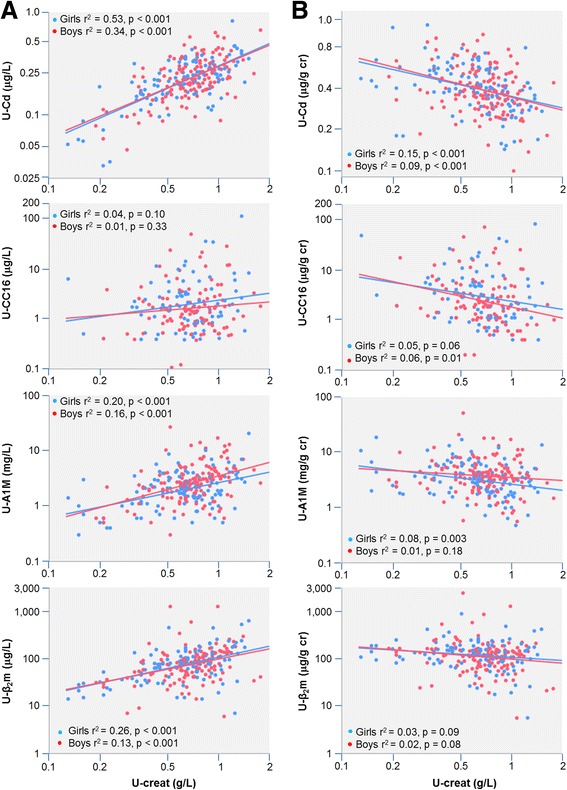
In a cross-sectional study involving 249 schoolchildren (mean age, 5.72 years; 138 boys), we measured the urine concentrations of cadmium, zinc, lead, albumin, alpha-microglobulin (A1M), retinol-binding protein, β-microglobulin and club cell protein (CC16). Determinants of U-Cd expressed per creatinine or adjusted to specific gravity were identified by multiple regression analyses.
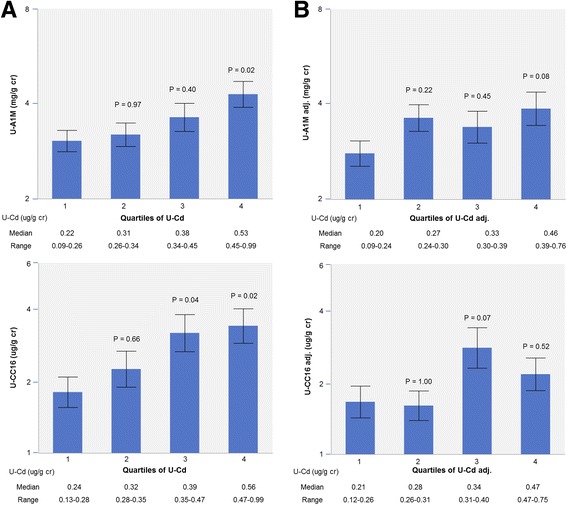
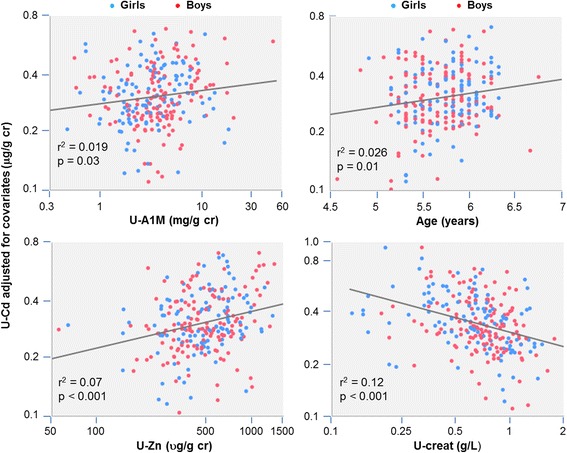
Girls and boys had similar median concentrations of U-Cd (0.22 and 0.24 μg/L, 0.33 and 0.35 μg/g creatinine, respectively). When models were run without including creatinine or specific gravity among independent variables, urinary zinc, urinary A1M and age emerged as the strongest predictors of U-Cd expressed per g creatinine or adjusted to SG. When adding creatinine among predictors, urinary creatinine emerged as an additional strong predictor correlating negatively with U-Cd per g creatinine. This strong residual influence of diuresis, not seen when adding specific gravity among predictors, linked U-Cd to U-A1M or U-CC16 through secondary associations mimicking those induced by Cd nephrotoxity.
In young children U-Cd largely varies with diuresis, zinc metabolism and urinary A1M. These physiological determinants, unrelated to Cd body burden, may confound the child renal and developmental outcomes associated with low-level U-Cd.
近期针对儿童的研究报告称,尿镉(U-Cd)作为镉体内负荷的生物标志物,与儿童肾功能障碍、生长发育迟缓及认知发育受损有关。然而,关于影响儿童尿镉水平且可能作为混杂因素的因素,我们知之甚少。
在一项横断面研究中,我们纳入了249名学童(平均年龄5.72岁;138名男孩),测量了他们尿液中镉、锌、铅、白蛋白、α-微球蛋白(A1M)、视黄醇结合蛋白、β-微球蛋白和克拉拉细胞蛋白(CC16)的浓度。通过多元回归分析确定了以肌酐为单位表示或根据比重调整后的尿镉的决定因素。
女孩和男孩的尿镉中位数浓度相似(分别为0.22和0.24μg/L,0.33和0.35μg/g肌酐)。当在自变量中不纳入肌酐或比重进行模型分析时,尿锌、尿A1M和年龄成为以g肌酐为单位表示或根据比重调整后的尿镉的最强预测因素。当在预测因素中加入肌酐时,尿肌酐成为另一个与每克肌酐尿镉呈负相关的强预测因素。在预测因素中加入比重时未观察到的这种强大的利尿残余影响,通过模仿镉肾毒性诱导的二次关联,将尿镉与尿A1M或尿CC16联系起来。
在幼儿中,尿镉很大程度上随利尿、锌代谢和尿A1M而变化。这些与镉体内负荷无关的生理决定因素,可能会混淆与低水平尿镉相关的儿童肾脏和发育结局。