Crivellaro Cinzia, Guglielmo Priscilla, De Ponti Elena, Elisei Federica, Guerra Luca, Magni Sonia, La Manna Maria, Di Martino Giampaolo, Landoni Claudio, Buda Alessandro
Department of Nuclear Medicine, ASST Monza, Monza University Milan-Bicocca, Milan Department of Medical Physics Department of Obstetrics and Gynecology, ASST Monza, Monza, Italy.
Medicine (Baltimore). 2017 Sep;96(38):e7943. doi: 10.1097/MD.0000000000007943.
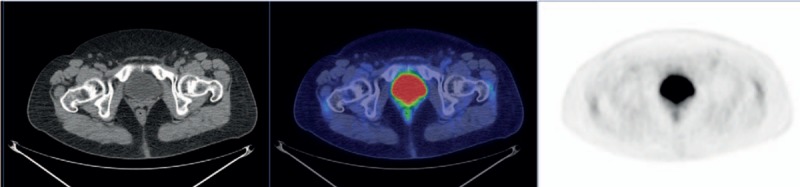
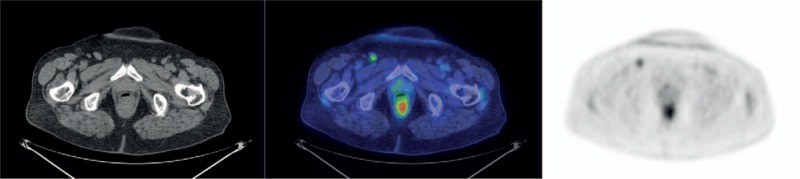
The aim of this study was to assess the role of 18F-FDG PET/CT in preoperative staging of vulvar cancer patients.29 pts (69 years, range 51-88) with vulvar cancer (clinical apparent stage I-II), underwent preoperative FDG-PET/CT scan followed by radical vulvectomy and bilateral (or monolateral in case of tumor >2 cm from midline) inguinal lymphadenectomy ± sentinel node biopsy. PET/CT images were analyzed in consensus and correlated to histological findings according to a pt-based and a groin-based analyses. SUVmax of the nodal uptake of each inguinal area (if present) was calculated and correlated to histological findings. The presence of distant metastases was also considered and confirmed.PET/CT analysis in consensus resulted negative at the inguinal LN level in 17 pts (10 true negative, 7 false negative) and positive in 12 pts (7 true positive, 5 false positive). Incidence of LN metastases resulted 48%. On pt-based analysis, sensitivity, specificity, accuracy, and negative and positive predictive value of PET/CT in detecting LN metastases were 50%, 67%, 59%, 59%, and 58%, respectively. On a groin-based analysis, considering overall 50 LN-sites, sensitivity, specificity, accuracy, and negative and positive predictive value of PET/CT were 53%, 85%, 73%, 67%, and 76%, respectively. The mean value of SUVmax was 6.1 (range 0.7-16.2) for metastatic nodes, whereas 1.6 (range 0.7 - 5.4) for negative lymph-nodes (P = .007). PET/CT detected pelvic (n = 1) and both pelvic/paraortic (n = 1) nodal metastases.In clinical early stage vulvar cancer FDG PET/CT showed low sensitivity and moderate specificity for N-staging; therefore, it is not an accurate tool for the nodal status assessment. PET/CT may not be cost-effective in detecting the rare event of distant metastases, but further studies are needed.
本研究的目的是评估18F-FDG PET/CT在外阴癌患者术前分期中的作用。29例(平均年龄69岁,范围51-88岁)临床I-II期外阴癌患者,术前行FDG-PET/CT扫描,随后行根治性外阴切除术及双侧(若肿瘤距中线>2 cm则为单侧)腹股沟淋巴结清扫术±前哨淋巴结活检。对PET/CT图像进行一致分析,并根据基于患者和基于腹股沟的分析与组织学结果进行关联。计算每个腹股沟区域(若存在)淋巴结摄取的SUVmax,并与组织学结果进行关联。同时考虑并确认远处转移的存在。一致分析显示,PET/CT在腹股沟淋巴结水平为阴性的有17例患者(10例真阴性,7例假阴性),阳性的有12例患者(7例真阳性,5例假阳性)。淋巴结转移发生率为48%。基于患者的分析中,PET/CT检测淋巴结转移的敏感性、特异性、准确性以及阴性和阳性预测值分别为50%、67%、59%、59%和58%。基于腹股沟的分析中,考虑总共50个淋巴结部位,PET/CT的敏感性、特异性、准确性以及阴性和阳性预测值分别为53%、85%、73%、67%和76%。转移淋巴结的SUVmax平均值为6.1(范围0.7-16.2),而阴性淋巴结为1.6(范围0.7-5.4)(P = 0.007)。PET/CT检测到盆腔(n = 1)和盆腔/腹主动脉旁(n = 1)淋巴结转移。在临床早期外阴癌中,FDG PET/CT对N分期显示出低敏感性和中等特异性;因此,它不是评估淋巴结状态的准确工具。PET/CT在检测罕见的远处转移事件方面可能不具有成本效益,但仍需要进一步研究。