Rockwood Neesha, Sirgel Frederick, Streicher Elizabeth, Warren Robin, Meintjes Graeme, Wilkinson Robert J
Department of Medicine, Imperial College.
Wellcome Centre for Infectious Diseases Research in Africa, Institute of Infectious Disease and Molecular Medicine, University of Cape Town, Cape Town.
J Infect Dis. 2017 Sep 15;216(6):632-640. doi: 10.1093/infdis/jix337.
We estimated the incidence of acquired isoniazid and rifampicin resistance in rifampicin-susceptible tuberculosis in a setting of high human immunodeficiency virus type 1 (HIV-1) infection and tuberculosis coprevalence.
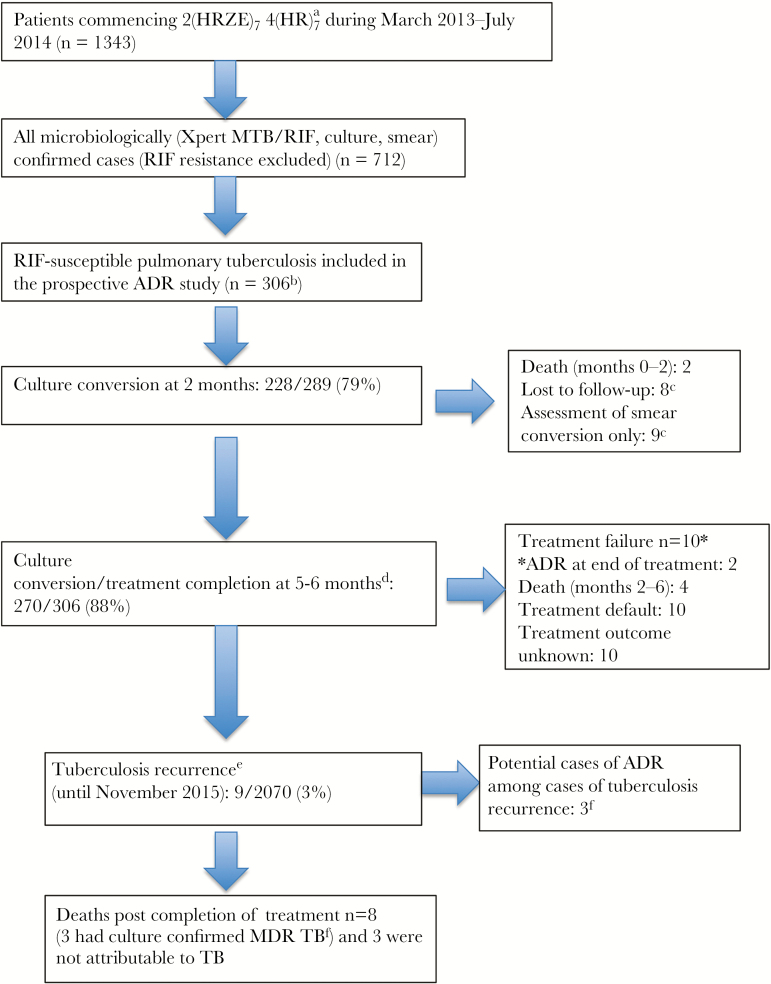
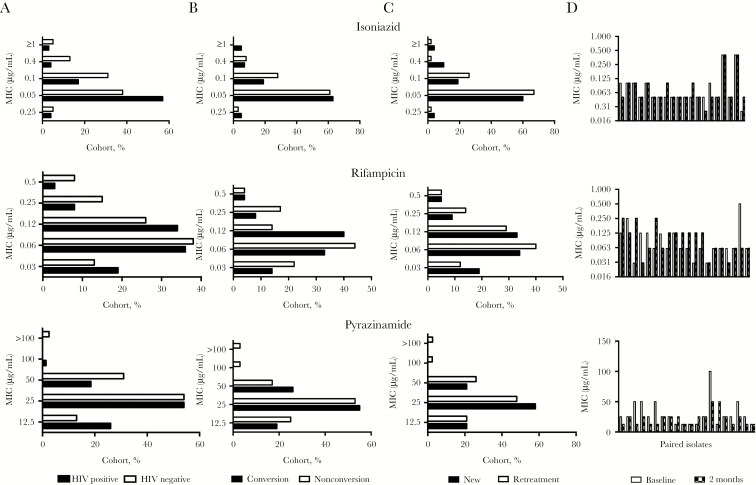
GeneXpert MTB/RIF-confirmed patients with rifampicin-susceptible tuberculosis were recruited at antituberculosis treatment initiation in Khayelitsha, South Africa. Liquid culture and adherence assessment were performed at 2 and 5-6 months. MTBDRplus was performed on mycobacteria-positive cultures to ascertain acquired drug resistance (ADR). Spoligotyping and whole-genome sequencing were performed to ascertain homogeneity between baseline isolates and isolates with ADR. Baseline isolates were retrospectively tested for isoniazid monoresistance. An electronic database review was performed to ascertain tuberculosis recurrences.
A total of 306 participants (62% with HIV-1 coinfection, of whom 71% received antiretroviral therapy) were recruited. Ascertainment of outcomes was complete for 284 participants. Five acquired a resistant Mycobacterium tuberculosis strain during or subsequent to treatment. One strain was confirmed to have ADR, 2 were confirmed as causing exogenous reinfection, and 2 were unrecoverable for genotyping. Incident ADR was estimated to have ranged from 0.3% (95% confidence interval [CI], .1%-1.9%; 1 of 284 participants) to 1% (95% CI, .2%-3%; 3 of 284 participants). Seventeen of 279 baseline isolates (6.1%; 95% CI, 3.6%-9.6%) had isoniazid monoresistance (13 of 17 had an inhA promoter mutation), but 0 of 17 had amplified resistance.
Treatment with standardized antituberculosis regimens dosed daily throughout, high uptake of antiretroviral therapy, and low prevalence of isoniazid monoresistance were associated with a low frequency of ADR.
在人类免疫缺陷病毒1型(HIV-1)感染率高且结核病共流行的情况下,我们估计了利福平敏感型结核病中获得性异烟肼和利福平耐药的发生率。
在南非开普敦Khayelitsha开始抗结核治疗时,招募GeneXpert MTB/RIF确诊的利福平敏感型结核病患者。在2个月和5 - 6个月时进行液体培养和依从性评估。对分枝杆菌阳性培养物进行MTBDRplus检测以确定获得性耐药(ADR)。进行间隔寡核苷酸分型(Spoligotyping)和全基因组测序以确定基线分离株与具有ADR的分离株之间的同源性。对基线分离株进行回顾性异烟肼单耐药检测。进行电子数据库审查以确定结核病复发情况。
共招募了306名参与者(62%合并HIV-1感染,其中71%接受抗逆转录病毒治疗)。284名参与者的结局确定完整。5名在治疗期间或治疗后获得耐药结核分枝杆菌菌株。1株被确认为具有ADR,2株被确认为引起外源性再感染,2株因基因分型无法恢复。估计ADR发生率为0.3%(95%置信区间[CI],0.1% - 1.9%;284名参与者中的1名)至1%(95% CI,0.2% - 3%;284名参与者中的3名)。279株基线分离株中有17株(6.1%;95% CI,3.6% - 9.6%)存在异烟肼单耐药(17株中有13株存在inhA启动子突变),但17株中0株存在扩增耐药。
全程每日给予标准化抗结核治疗方案、抗逆转录病毒治疗的高接受率以及异烟肼单耐药的低患病率与ADR的低发生率相关。