Chandra Sadanandavalli Retnaswami, Viswanathan Lakshminarayanapuram Gopal, Pai Anupama Ramakanth, Wahatule Rahul, Alladi Suvarna
Department of Neurology, National Institute of Mental Health and Neurosciences, Bengaluru, Karnataka, India.
Department of Neuromicrobiology, National Institute of Mental Health and Neurosciences, Bengaluru, Karnataka, India.
J Neurosci Rural Pract. 2017 Aug;8(Suppl 1):S66-S71. doi: 10.4103/jnrp.jnrp_100_17.
Dementias are fairly slowly progressive degenerative diseases of brain for which treatment options are very less and carry a lot of burden on family and society. A small percentage of them are rapidly progressive and mostly carry a different course outcome. However, there are no definite criteria other than the time line for these patients.
The aim of this was to identify and categorize the causes and course of rapidly progressive dementias seen in our center.
Patients who presented with rapid deterioration of cognitive functions within weeks to 1 year between 2011 and December 2016 were evaluated.
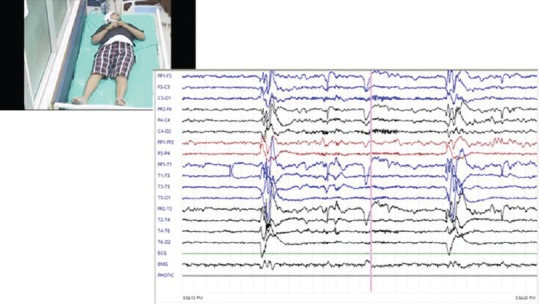
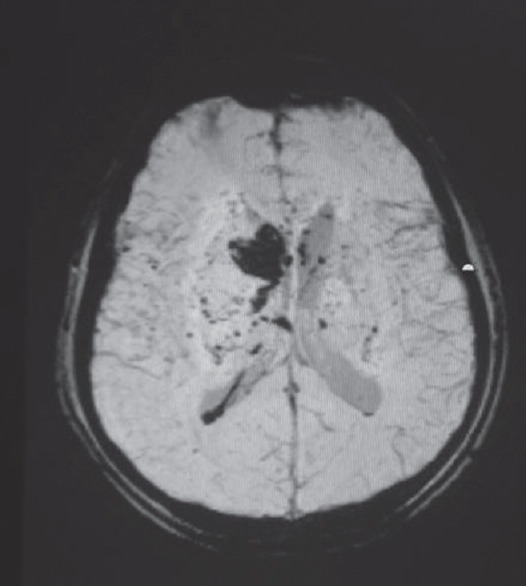
All patients underwent all mandatory tests for dementia including brain imaging. Complete vasculitis workup, autoimmune encephalitis profile including Voltage Gated Potassium Channel, N-methyl-D-aspartic acid receptor, glutamic acid-decarboxylase, thyroid-peroxidase antibody, cerebrospinal fluid, and other special tests such as duodenal biopsy and paraneoplastic workup were done based on clinical indications.
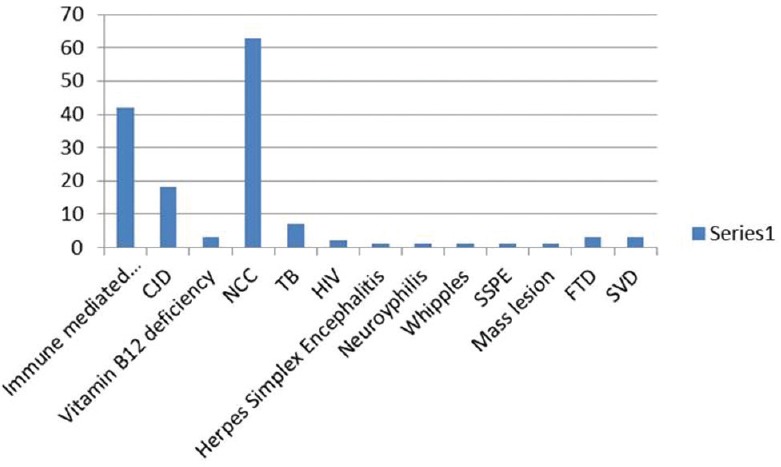
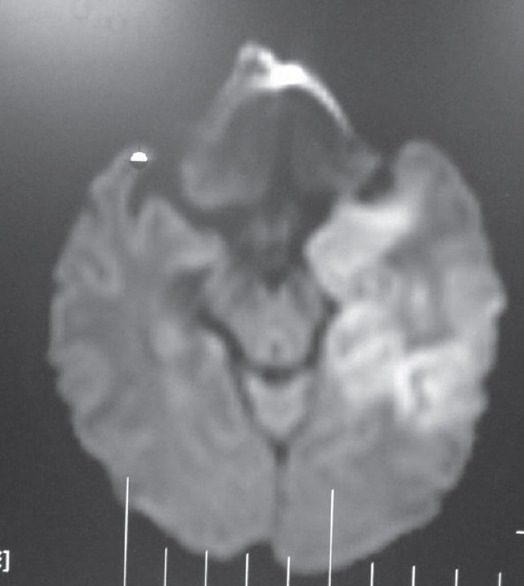
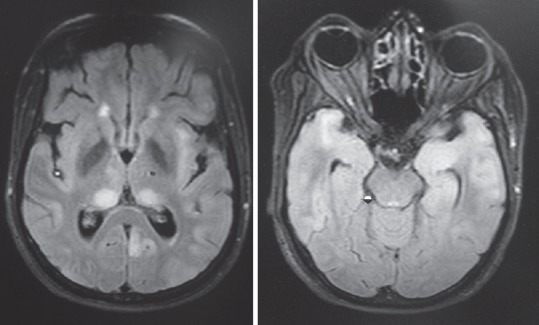
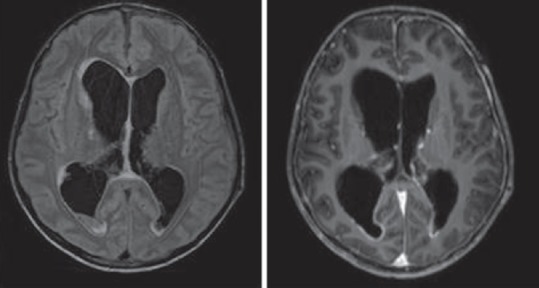
Out of 144 patients 42 had immune-mediated encephalopathy, 18 had Creutzfeldt-Jakob disease, 3 had Vitamin B12 deficiency, 63 had infection with neurocysticercosis, 7 had tuberculosis, 2 had HIV, 1 had herpes simplex encephalitis, 1 had neurosyphilis, 1 Whipples disease, 1 had Subacute Sclerosing Panencephalitis, 1 had Mass lesion, 3 had Frontotemporal dementia, and 3 had small vessel disease. Good majority of these patients have infective and immune-mediated causes and less number belong to degenerative group. Therefore, caution is needed to look for treatable cause as it carries a different treatment options and outcome.
痴呆症是大脑相当缓慢进展的退行性疾病,治疗选择非常有限,给家庭和社会带来沉重负担。其中一小部分进展迅速,且大多有不同的病程结果。然而,除了病程时间线外,这些患者没有明确的标准。
本研究的目的是识别并分类在我们中心所见的快速进展性痴呆的病因和病程。
对2011年至2016年12月期间在数周内至1年内认知功能迅速恶化的患者进行评估。
所有患者均接受了痴呆症的所有强制性检查,包括脑部成像。根据临床指征,进行了全面的血管炎检查、自身免疫性脑炎检测,包括电压门控钾通道、N-甲基-D-天冬氨酸受体、谷氨酸脱羧酶、甲状腺过氧化物酶抗体、脑脊液检测,以及其他特殊检查,如十二指肠活检和副肿瘤检查。
144例患者中,42例患有免疫介导性脑病,18例患有克雅氏病,3例患有维生素B12缺乏症,63例患有神经囊尾蚴病感染,7例患有结核病,2例患有艾滋病,1例患有单纯疱疹性脑炎,1例患有神经梅毒,1例患有惠普尔病,1例患有亚急性硬化性全脑炎,1例患有占位性病变,3例患有额颞叶痴呆,3例患有小血管疾病。这些患者中绝大多数有感染性和免疫介导性病因,属于退行性病变组的较少。因此,需要谨慎寻找可治疗的病因,因为其治疗选择和结果不同。