Ueno Tatsuya, Kon Tomoya, Kurihara Ai-Ichiro, Tomiyama Masahiko
Department of Neurology, Aomori Prefectural Central Hospital, Japan.
Department of Neurology, Aomori Rosai Hospital, Japan.
Intern Med. 2017 Nov 1;56(21):2929-2932. doi: 10.2169/internalmedicine.8824-17. Epub 2017 Sep 25.
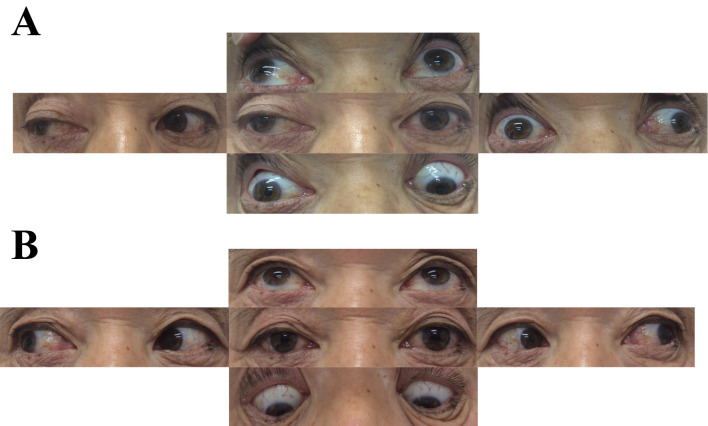
Unilateral oculomotor nerve palsy can result from various neurological disorders. We herein report the case of a 68-year-old man with complete unilateral oculomotor nerve palsy following campylobacter infection. Based on the antecedent infection and the patient's decreased tendon reflexes, incomplete Miller Fisher syndrome (MFS) without ataxia was suspected. His serum tested positive for anti-GQ1b antibodies. He recovered over a period of 87 days without immunotherapy. We conclude that incomplete MFS following campylobacter infection can cause unilateral oculomotor nerve palsy without ataxia. Mild MFS should be considered in patients presenting with unilateral isolated ophthalmoplegia and decreased tendon reflexes.
单侧动眼神经麻痹可由多种神经系统疾病引起。我们在此报告一例68岁男性,在感染弯曲杆菌后出现完全性单侧动眼神经麻痹。基于先前的感染以及患者腱反射减弱,怀疑为无共济失调的不完全性米勒·费希尔综合征(MFS)。他的血清抗GQ1b抗体检测呈阳性。未经免疫治疗,他在87天内康复。我们得出结论,弯曲杆菌感染后的不完全性MFS可导致无共济失调的单侧动眼神经麻痹。对于出现单侧孤立性眼肌麻痹和腱反射减弱的患者,应考虑轻度MFS。