Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, USA.
Department of Medicine, Institut Gustave Roussy and Paris Sud University, Paris, France.
Ann Oncol. 2017 Oct 1;28(10):2581-2587. doi: 10.1093/annonc/mdx339.
The BRIM-3 trial showed improved progression-free survival (PFS) and overall survival (OS) for vemurafenib compared with dacarbazine in treatment-naive patients with BRAFV600 mutation-positive metastatic melanoma. We present final OS data from BRIM-3.
Patients were randomly assigned in a 1 : 1 ratio to receive vemurafenib (960 mg twice daily) or dacarbazine (1000 mg/m2 every 3 weeks). OS and PFS were co-primary end points. OS was assessed in the intention-to-treat population, with and without censoring of data for dacarbazine patients who crossed over to vemurafenib.
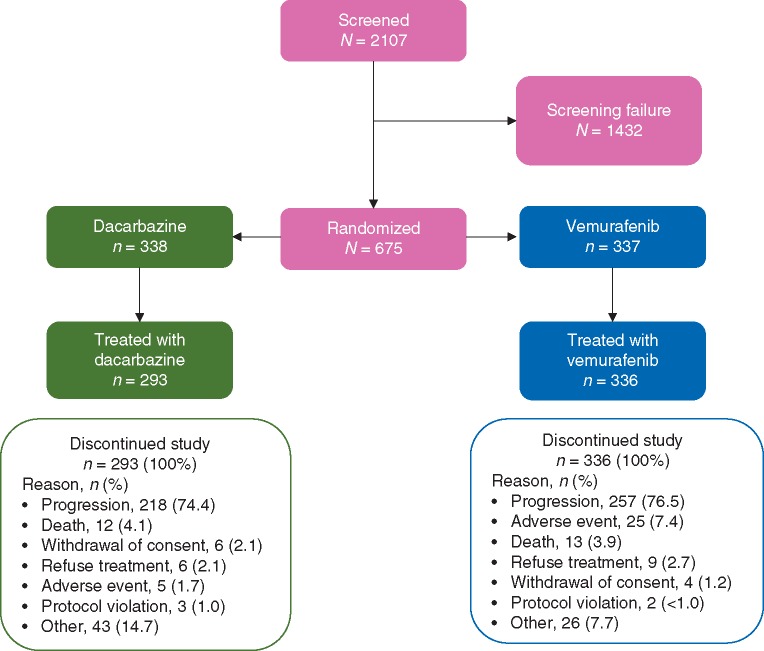
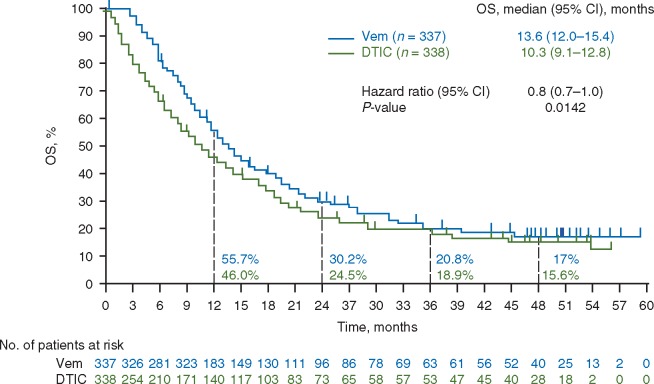
Between 4 January 2010 and 16 December 2010, a total of 675 patients were randomized to vemurafenib (n = 337) or dacarbazine (n = 338, of whom 84 crossed over to vemurafenib). At the time of database lock (14 August 2015), median OS, censored at crossover, was significantly longer for vemurafenib than for dacarbazine {13.6 months [95% confidence interval (CI) 12.0-15.4] versus 9.7 months [95% CI 7.9-12.8; hazard ratio (HR) 0.81 [95% CI 0.67-0.98]; P = 0.03}, as was median OS without censoring at crossover [13.6 months (95% CI 12.0-15.4) versus 10.3 months (95% CI 9.1-12.8); HR 0.81 (95% CI 0.68-0.96); P = 0.01]. Kaplan-Meier estimates of OS rates for vemurafenib versus dacarbazine were 56% versus 46%, 30% versus 24%, 21% versus 19% and 17% versus 16% at 1, 2, 3 and 4 years, respectively. Overall, 173 of the 338 patients (51%) in the dacarbazine arm and 175 of the 337 (52%) of those in the vemurafenib arm received subsequent anticancer therapies, most commonly ipilimumab. Safety data were consistent with the primary analysis.
Vemurafenib continues to be associated with improved median OS in the BRIM-3 trial after extended follow-up. OS curves converged after ≈3 years, likely as a result of crossover from dacarbazine to vemurafenib and receipt of subsequent anticancer therapies.
CLINICALTRIALS.GOV: NCT01006980.
BRIM-3 试验表明,与达卡巴嗪相比,维莫非尼可改善 BRAFV600 突变阳性转移性黑色素瘤初治患者的无进展生存期(PFS)和总生存期(OS)。我们报告 BRIM-3 的最终 OS 数据。
患者按 1:1 的比例随机分配接受维莫非尼(960mg 每日两次)或达卡巴嗪(1000mg/m2,每 3 周)治疗。OS 和 PFS 是共同的主要终点。在意向治疗人群中评估 OS,包括和不包括达卡巴嗪组交叉至维莫非尼组患者的数据删失。
2010 年 1 月 4 日至 2010 年 12 月 16 日,共 675 例患者被随机分配至维莫非尼组(n=337)或达卡巴嗪组(n=338,其中 84 例交叉至维莫非尼组)。在数据库锁定(2015 年 8 月 14 日)时,中位 OS(交叉时删失)维莫非尼组显著长于达卡巴嗪组{13.6 个月[95%置信区间(CI)12.0-15.4]与 9.7 个月[95% CI 7.9-12.8;风险比(HR)0.81[95% CI 0.67-0.98];P=0.03},无交叉时删失的中位 OS 也更长{13.6 个月(95% CI 12.0-15.4)与 10.3 个月(95% CI 9.1-12.8);HR 0.81(95% CI 0.68-0.96);P=0.01}。维莫非尼与达卡巴嗪的 OS 率Kaplan-Meier 估计值分别为 56%比 46%、30%比 24%、21%比 19%和 17%比 16%,分别在 1、2、3 和 4 年时。达卡巴嗪组 338 例患者(51%)和维莫非尼组 337 例患者(52%)中,173 例和 175 例患者接受了后续抗癌治疗,最常见的是伊匹单抗。安全性数据与主要分析一致。
在延长随访后,维莫非尼在 BRIM-3 试验中继续与改善的中位 OS 相关。OS 曲线在约 3 年后趋同,可能是由于达卡巴嗪交叉至维莫非尼以及接受后续抗癌治疗所致。
临床试验.gov:NCT01006980。