Department of Cardiovascular Surgery, University Hospital of Schleswig-Holstein, Kiel, Germany
Department of Cardiovascular Surgery, University Hospital of Schleswig-Holstein, Kiel, Germany.
J Am Heart Assoc. 2017 Oct 3;6(10):e005498. doi: 10.1161/JAHA.117.005498.
The optimal timing of coronary artery bypass grafting (CABG) in clinically stable patients with acute myocardial infarction who are unsuitable for percutaneous coronary intervention is unclear. We report our experience with early CABG in these patients.
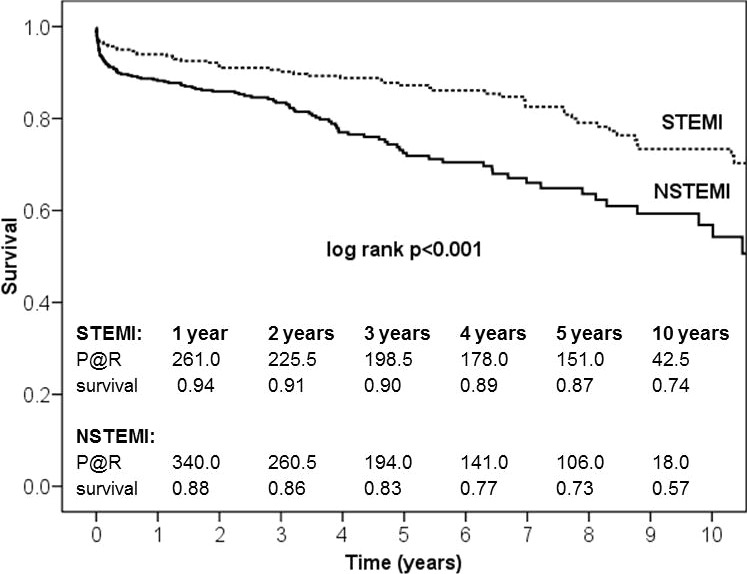
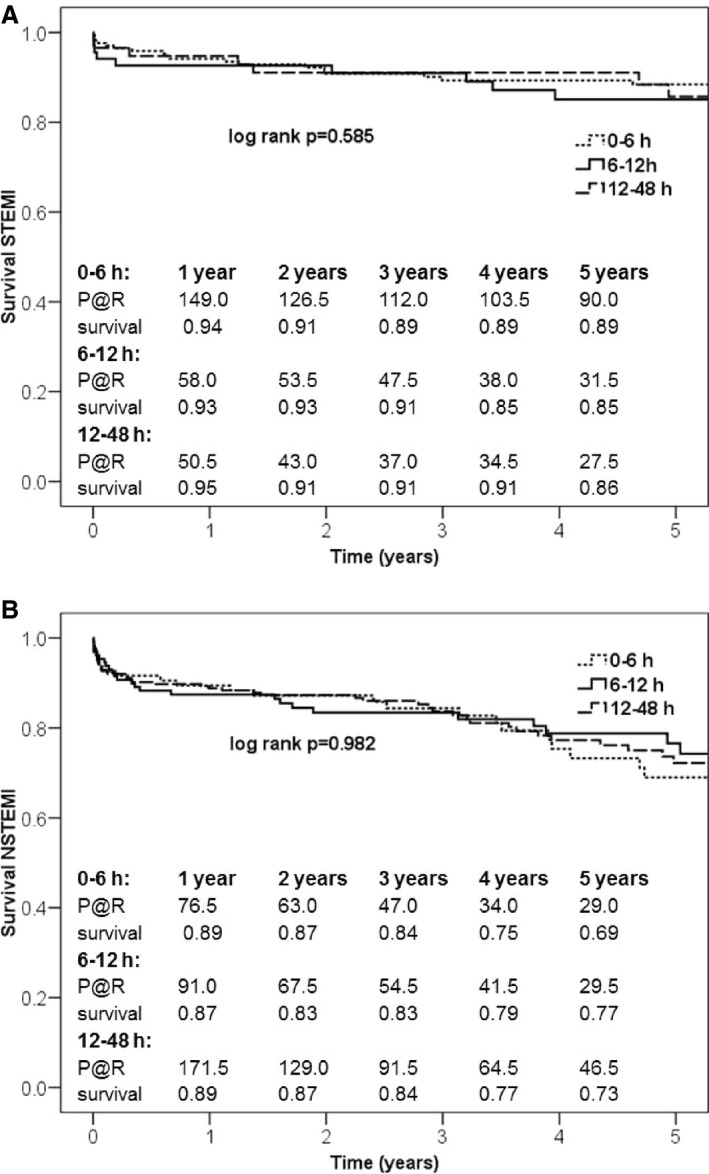
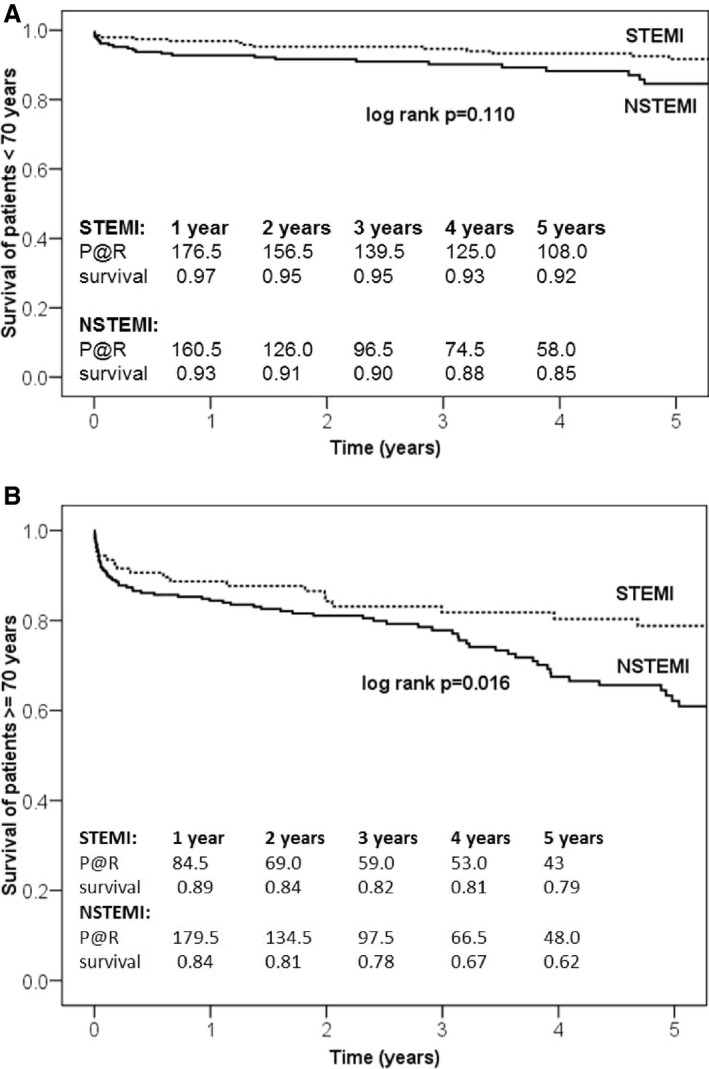
Between January 2001 and May 2015, 766 patients with ST-segment-elevation myocardial infarction (STEMI, n=305) or non-STEMI (NSTEMI, n=461) not including cardiogenic shock underwent CABG within 48 hours at our department. STEMI patients were younger than non-STEMI patients (age 65 years [range: 58-72] versus 70 years [range: 62-75], <0.001) with a lower EuroSCORE II (4.12 [range: 2.75-5.81] versus 4.58 [range: 2.80-7.74], =0.009). STEMI patients had undergone preoperative percutaneous coronary intervention more often (20.3% versus 7.8%, <0.001). Time to surgery was shorter in STEMI compared with non-STEMI patients (5.0 hours [range: 3.2-8.8] versus 11.7 hours [range: 6.4-22.0], <0.001). No significant differences concerning arterial graft use (93.8% versus 94.8%, =0.540) or complete revascularization (87.5% versus 83.4%, =0.121) were observed. The rate of strokes did not differ between the groups (2.0% versus 3.9%, =0.134). Thirty-day mortality was lower in STEMI patients (2.7% versus 6.6% =0.018), especially when CABG was performed within 6 hours (1.8% versus 7.1%, =0.041). Survival of STEMI and non-STEMI patients was 94% versus 88% after 1 year (<0.001), 87% versus 73% after 5 years (<0.001), and 74% versus 57% after 10 years (<0.001). Independent predictors of 30-day and long-term mortality included preoperatively increased lactate values, age, atrial fibrillation, and reduced left ventricular function.
Stable STEMI patients showed a lower rate of perioperative complications and better survival compared with non-STEMI patients when CABG was performed within 48 hours.
对于不适合经皮冠状动脉介入治疗的急性心肌梗死且临床稳定的患者,冠状动脉旁路移植术(CABG)的最佳时机尚不清楚。我们报告了在这些患者中进行早期 CABG 的经验。
2001 年 1 月至 2015 年 5 月,我院共对 766 例 ST 段抬高型心肌梗死(STEMI,n=305)或非 ST 段抬高型心肌梗死(NSTEMI,n=461)患者进行了 CABG,这些患者在发病 48 小时内接受了 CABG。与 NSTEMI 患者相比,STEMI 患者更年轻(年龄 65 岁[范围:58-72] vs. 70 岁[范围:62-75],<0.001),EuroSCORE II 评分较低(4.12[范围:2.75-5.81] vs. 4.58[范围:2.80-7.74],=0.009)。STEMI 患者术前接受经皮冠状动脉介入治疗的比例更高(20.3% vs. 7.8%,<0.001)。与 NSTEMI 患者相比,STEMI 患者的手术时间更短(5.0 小时[范围:3.2-8.8] vs. 11.7 小时[范围:6.4-22.0],<0.001)。两组之间在动脉移植物的使用(93.8% vs. 94.8%,=0.540)或完全血运重建(87.5% vs. 83.4%,=0.121)方面没有显著差异。两组之间的卒中发生率无差异(2.0% vs. 3.9%,=0.134)。STEMI 患者的 30 天死亡率较低(2.7% vs. 6.6%=0.018),尤其是当 CABG 在 6 小时内进行时(1.8% vs. 7.1%=0.041)。STEMI 和 NSTEMI 患者在 1 年时的生存率分别为 94%和 88%(<0.001),5 年时分别为 87%和 73%(<0.001),10 年时分别为 74%和 57%(<0.001)。30 天和长期死亡率的独立预测因素包括术前乳酸值升高、年龄、心房颤动和左心室功能降低。
与 NSTEMI 患者相比,在发病 48 小时内进行 CABG 的 STEMI 患者围手术期并发症发生率较低,生存预后较好。