Department of Radiology, Dalio Institute of Cardiovascular Imaging, NewYork-Presbyterian Hospital and Weill Cornell Medicine, 413 E. 69th Street, Suite 108, New York, NY 10021, USA.
Division of Cardiology, Severance Cardiovascular Hospital and Severance Biomedical Science Institute, Yonsei University College of Medicine, Yonsei University Health System, Seoul, South Korea.
Eur Heart J Cardiovasc Imaging. 2018 Jun 1;19(6):675-683. doi: 10.1093/ehjci/jex150.
Coronary computed tomography angiography (CCTA) and coronary artery calcium score (CACS) have prognostic value for coronary artery disease (CAD) events beyond traditional risk assessment. Age is a risk factor with very high weight and little is known regarding the incremental value of CCTA over CAC for predicting cardiac events in older adults.
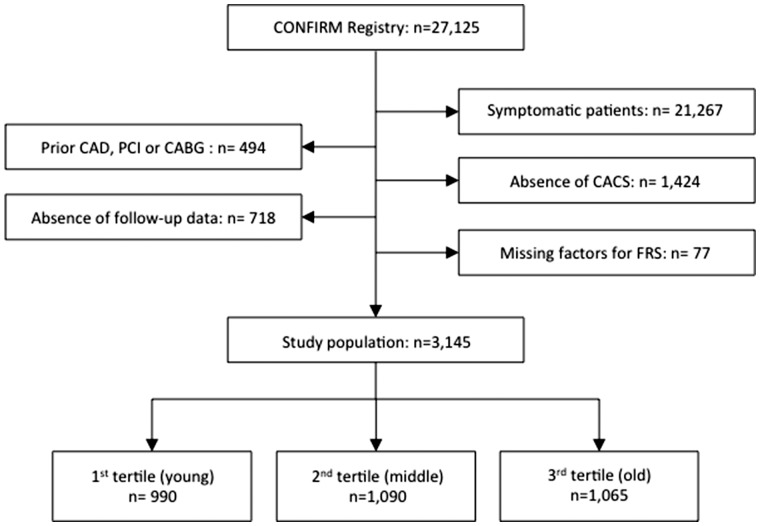
Of 27 125 individuals undergoing CCTA, a total of 3145 asymptomatic adults were identified. This study sample was categorized according to tertiles of age (cut-off points: 52 and 62 years). CAD severity was classified as 0, 1-49, and ≥50% maximal stenosis in CCTA, and further categorized according to number of vessels ≥50% stenosis. The Framingham 10-year risk score (FRS) and CACS were employed as major covariates. Major adverse cardiovascular events (MACE) were defined as a composite of all-cause death or non-fatal MI. During a median follow-up of 26 months (interquartile range: 18-41 months), 59 (1.9%) MACE occurred. For patients in the top age tertile, CCTA improved discrimination beyond a model included FRS and CACS (C-statistic: 0.75 vs. 0.70, P-value = 0.015). Likewise, the addition of CCTA improved category-free net reclassification (cNRI) of MACE in patients within the highest age tertile (e.g. cNRI = 0.75; proportion of events/non-events reclassified were 50 and 25%, respectively; P-value <0.05, all). CCTA displayed no incremental benefit beyond FRS and CACS for prediction of MACE in the lower age tertiles.
CCTA provides added prognostic value beyond cardiac risk factors and CACS for the prediction of MACE in asymptomatic older adults.
冠状动脉计算机断层扫描血管造影(CCTA)和冠状动脉钙评分(CACS)在预测冠状动脉疾病(CAD)事件方面具有比传统风险评估更重要的预后价值。年龄是一个具有很高权重的危险因素,对于 CACS 预测老年人心脏事件的增量价值,人们知之甚少。
在 27125 名接受 CCTA 的个体中,共确定了 3145 名无症状成年人。根据年龄三分位数(截止点:52 岁和 62 岁)对本研究样本进行分类。CCTA 中 CAD 严重程度分为 0、1-49 和≥50%最大狭窄,并根据≥50%狭窄的血管数量进一步分类。Framingham 10 年风险评分(FRS)和 CACS 作为主要协变量。主要不良心血管事件(MACE)定义为全因死亡或非致死性心肌梗死的复合事件。在中位数为 26 个月(四分位间距:18-41 个月)的随访期间,发生 59 例(1.9%)MACE。对于处于最高年龄三分位数的患者,CCTA 提高了包含 FRS 和 CACS 的模型的区分度(C 统计量:0.75 比 0.70,P 值=0.015)。同样,在最高年龄三分位数的患者中,CCTA 增加了 MACE 的无分类净重新分类(cNRI)(例如,cNRI=0.75;事件/非事件重新分类的比例分别为 50%和 25%,P 值均<0.05)。在年龄较低的三分位数中,CCTA 对预测 MACE 没有超过 FRS 和 CACS 的额外获益。
CCTA 为预测无症状老年人心血管事件提供了除心脏危险因素和 CACS 之外的预后价值。