Bailie Ross, Matthews Veronica, Larkins Sarah, Thompson Sandra, Burgess Paul, Weeramanthri Tarun, Bailie Jodie, Cunningham Frances, Kwedza Ru, Clark Louise
University Centre for Rural Health-North Coast, School of Rural Health, University of Sydney, Lismore, New South Wales, Australia.
College of Medicine and Dentistry, James Cook University, Townsville, Queensland, Australia.
BMJ Open. 2017 Oct 5;7(10):e016626. doi: 10.1136/bmjopen-2017-016626.
To examine the impact of state/territory policy support on (1) uptake of evidence-based continuous quality improvement (CQI) activities and (2) quality of care for Indigenous Australians.
Mixed-method comparative case study methodology, drawing on quality-of-care audit data, documentary evidence of policies and strategies and the experience and insights of stakeholders involved in relevant CQI programmes. We use multilevel linear regression to analyse jurisdictional differences in quality of care.
Indigenous primary healthcare services across five states/territories of Australia.
175 Indigenous primary healthcare services.
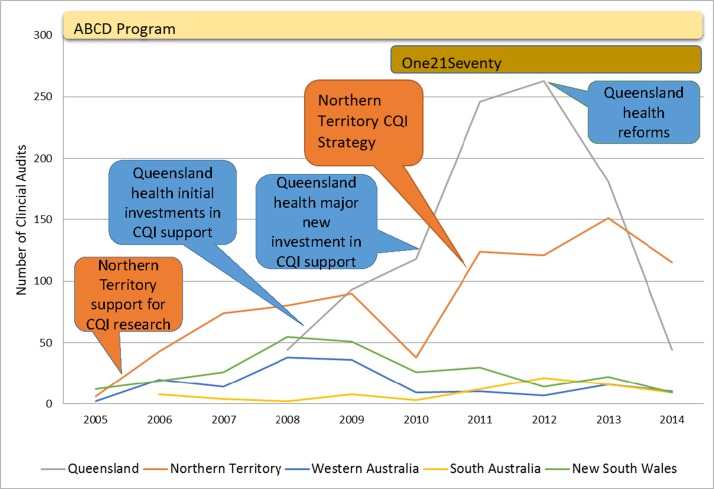
A range of national and state/territory policy and infrastructure initiatives to support CQI, including support for applied research. PRIMARY AND SECONDARY OUTCOME MEASURES: (i) Trends in the consistent uptake of evidence-based CQI tools available through a research-based CQI initiative (the Audit and Best Practice in Chronic Disease programme) and (ii) quality of care (as reflected in adherence to best practice guidelines).
Progressive uptake of evidence-based CQI activities and steady improvements or maintenance of high-quality care occurred where there was long-term policy and infrastructure support for CQI. Where support was provided but not sustained there was a rapid rise and subsequent fall in relevant CQI activities.
Health authorities should ensure consistent and sustained policy and infrastructure support for CQI to enable wide-scale and ongoing improvement in quality of care and, subsequently, health outcomes. It is not sufficient for improvement initiatives to rely on local service managers and clinicians, as their efforts are strongly mediated by higher system-level influences.
探讨州/领地政策支持对(1)循证持续质量改进(CQI)活动的采用情况以及(2)澳大利亚原住民医疗服务质量的影响。
采用混合方法比较案例研究方法,利用医疗服务质量审计数据、政策和策略的文献证据以及参与相关CQI项目的利益相关者的经验和见解。我们使用多层线性回归分析医疗服务质量的辖区差异。
澳大利亚五个州/领地的原住民初级医疗服务机构。
175家原住民初级医疗服务机构。
一系列支持CQI的国家和州/领地政策及基础设施举措,包括对应用研究的支持。
(i)通过一项基于研究的CQI举措(慢性病审计与最佳实践项目)可获得的循证CQI工具的持续采用趋势,以及(ii)医疗服务质量(以遵循最佳实践指南来体现)。
在对CQI有长期政策和基础设施支持的地方,循证CQI活动逐步得到采用,高质量医疗服务稳步改善或维持在较高水平。在提供了支持但未持续的地方,相关CQI活动迅速增加,随后下降。
卫生当局应确保对CQI提供持续一致的政策和基础设施支持,以使医疗服务质量得到广泛且持续的改善,进而改善健康结局。改进举措仅依靠地方服务管理人员和临床医生是不够的,因为他们的努力受到更高系统层面因素的强烈影响。