Aggarwal Ajay, Lewis Daniel, Mason Malcolm, Purushotham Arnie, Sullivan Richard, van der Meulen Jan
Department of Health Services Research & Policy, London School of Hygiene & Tropical Medicine, London, UK; Clinical Effectiveness Unit, Royal College of Surgeons of England, London, UK.
Department of Social and Environment Health Research, London School of Hygiene & Tropical Medicine, London, UK.
Lancet Oncol. 2017 Nov;18(11):1445-1453. doi: 10.1016/S1470-2045(17)30572-7. Epub 2017 Oct 3.
There is a scarcity of evidence about the role of patient choice and hospital competition policies on surgical cancer services. Previous evidence has shown that patients are prepared to bypass their nearest cancer centre to receive surgery at more distant centres that better meet their needs. In this national, population-based study we investigated the effect of patient mobility and hospital competition on service configuration and technology adoption in the National Health Service (NHS) in England, using prostate cancer surgery as a model.
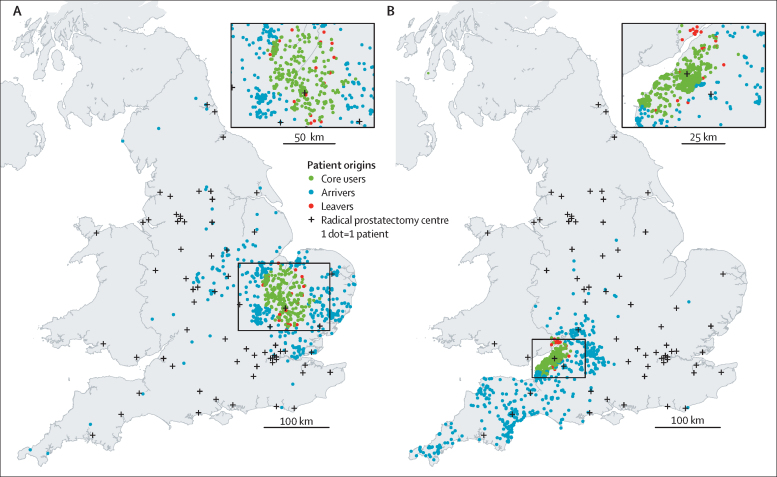
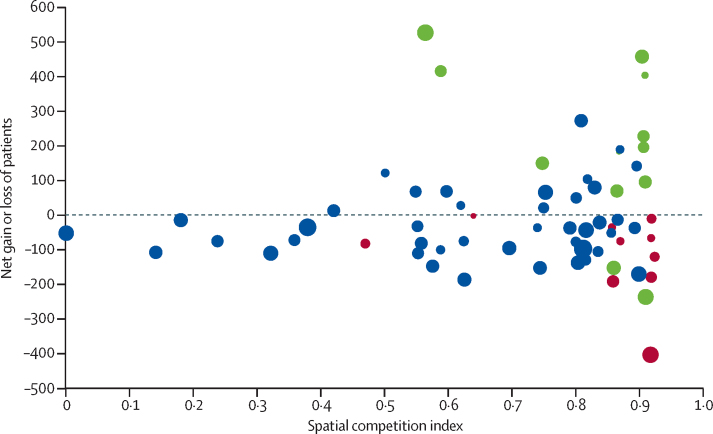
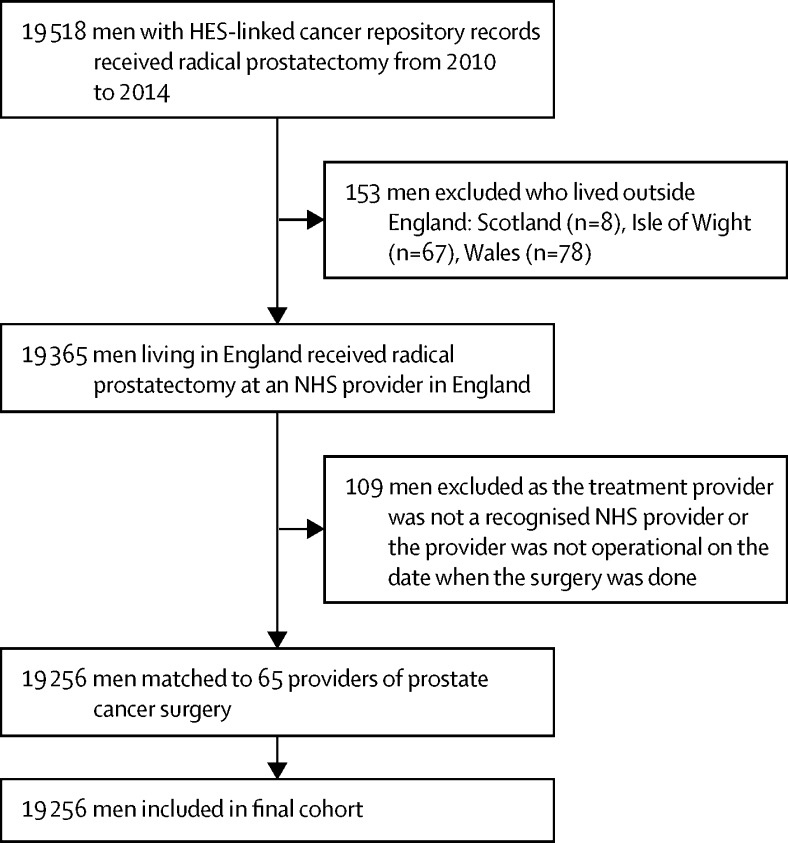
We mapped all patients in England who underwent radical prostatectomy between Jan 1, 2010, and Dec 31, 2014, according to place of residence and treatment location. For each radical prostatectomy centre we analysed the effect of hospital competition (measured by use of a spatial competition index [SCI], with a score of 0 indicating weakest competition and 1 indicating strongest competition) and the effect of being an established robotic radical prostatectomy centre at the start of 2010 on net gains or losses of patients (difference between number of patients treated in a centre and number expected based on their residence), and the likelihood of closing their radical prostatectomy service.
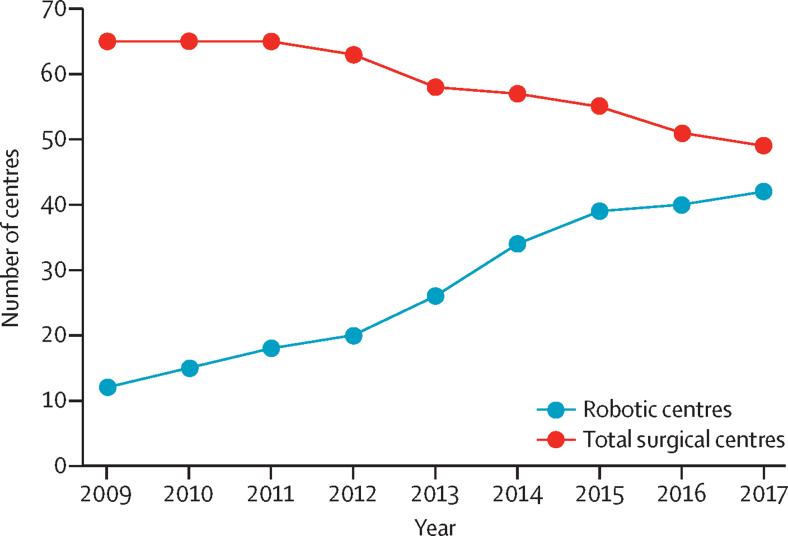
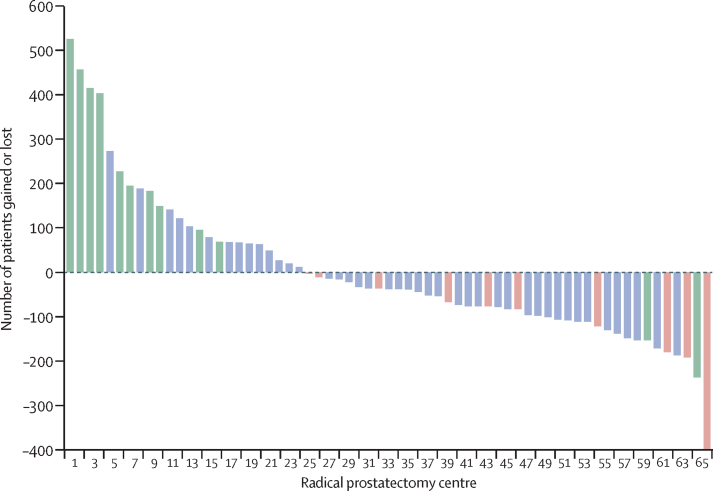
Between Jan 1, 2010, and Dec 31, 2014, 19 256 patients underwent radical prostatectomy at an NHS provider in England. Of the 65 radical prostatectomy centres open at the start of the study period, 23 (35%) had a statistically significant net gain of patients during 2010-14. Ten (40%) of these 23 were established robotic centres. 37 (57%) of the 65 centres had a significant net loss of patients, of which two (5%) were established robotic centres and ten (27%) closed their radical prostatectomy service during the study period. Radical prostatectomy centres that closed were more likely to be located in areas with stronger competition (highest SCI quartile [0·87-0·92]; p=0·0081) than in areas with weaker competition. No robotic surgery centre closed irrespective of the size of net losses of patients. The number of centres performing robotic surgery increased from 12 (18%) of the 65 centres at the beginning of 2010 to 39 (71%) of 55 centres open at the end of 2014.
Competitive factors, in addition to policies advocating centralisation and the requirement to do minimum numbers of surgical procedures, have contributed to large-scale investment in equipment for robotic surgery without evidence of superior outcomes and contributed to the closure of cancer surgery units. If quality performance and outcome indicators are not available to guide patient choice, these policies could threaten health services' ability to deliver equitable and affordable cancer care.
National Institute for Health Research.
关于患者选择和医院竞争政策对外科癌症服务的作用,证据不足。先前的证据表明,患者愿意绕过最近的癌症中心,前往更远处能更好满足其需求的中心接受手术。在这项基于全国人口的研究中,我们以前列腺癌手术为模型,调查了患者流动和医院竞争对英格兰国民医疗服务体系(NHS)服务配置和技术采用的影响。
我们根据居住地和治疗地点,绘制了2010年1月1日至2014年12月31日期间在英格兰接受根治性前列腺切除术的所有患者的地图。对于每个根治性前列腺切除术中心,我们分析了医院竞争的影响(通过空间竞争指数[SCI]衡量,分数为0表示竞争最弱,1表示竞争最强)以及在2010年初成为既定的机器人根治性前列腺切除术中心对患者净增减(中心治疗的患者数量与基于其居住地预期的患者数量之差)的影响,以及关闭其根治性前列腺切除术服务的可能性。
在2010年1月1日至2014年12月31日期间,19256名患者在英格兰的NHS医疗机构接受了根治性前列腺切除术。在研究期开始时开放的65个根治性前列腺切除术中心中,23个(35%)在2010 - 2014年期间患者净增加具有统计学意义。这23个中心中有10个(40%)是既定的机器人手术中心。65个中心中有37个(57%)患者净减少显著,其中2个(5%)是既定的机器人手术中心,10个(27%)在研究期间关闭了其根治性前列腺切除术服务。关闭的根治性前列腺切除术中心比竞争较弱地区的中心更有可能位于竞争较强的地区(最高SCI四分位数[0.87 - 0.92];p = 0.0081)。无论患者净损失规模如何,没有机器人手术中心关闭。进行机器人手术的中心数量从2010年初65个中心中的12个(18%)增加到2014年底开放的55个中心中的39个(71%)。
除了主张集中化的政策和进行最低数量外科手术的要求外,竞争因素导致了对机器人手术设备的大规模投资,但没有证据表明结果更优,还导致了癌症手术科室的关闭。如果没有质量绩效和结果指标来指导患者选择,这些政策可能会威胁到卫生服务机构提供公平且负担得起的癌症护理的能力。
国家卫生研究院。