Macintyre Fiona, Adoke Yeka, Tiono Alfred B, Duong Tran Thanh, Mombo-Ngoma Ghyslain, Bouyou-Akotet Marielle, Tinto Halidou, Bassat Quique, Issifou Saadou, Adamy Marc, Demarest Helen, Duparc Stephan, Leroy Didier, Laurijssens Bart E, Biguenet Sophie, Kibuuka Afizi, Tshefu Antoinette Kitoto, Smith Melnick, Foster Chanelle, Leipoldt Illse, Kremsner Peter G, Phuc Bui Quang, Ouedraogo Alphonse, Ramharter Michael
Medicines for Malaria Venture, Geneva, Switzerland.
Infectious Diseases Research Collaboration, Tororo Hospital, Tororo, Uganda.
BMC Med. 2017 Oct 9;15(1):181. doi: 10.1186/s12916-017-0940-3.
The clinical development of a single encounter treatment for uncomplicated malaria has the potential to significantly improve the effectiveness of antimalarials. Exploratory data suggested that the combination of artefenomel and piperaquine phosphate (PQP) has the potential to achieve satisfactory cure rates as a single dose therapy. The primary objective of the study was to determine whether a single dose of artefenomel (800 mg) plus PQP in ascending doses is an efficacious treatment for uncomplicated Plasmodium falciparum malaria in the 'target' population of children ≤ 5 years of age in Africa as well as Asian patients of all ages.
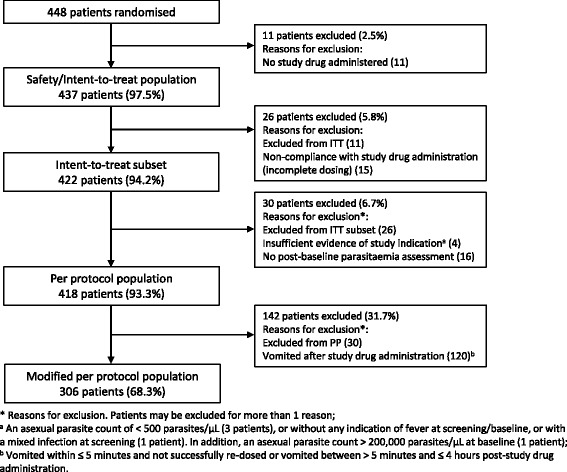
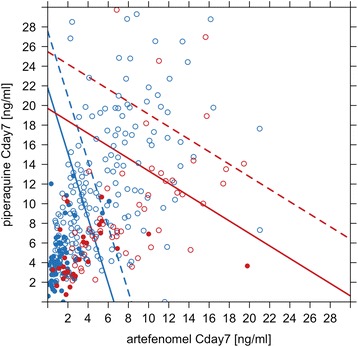
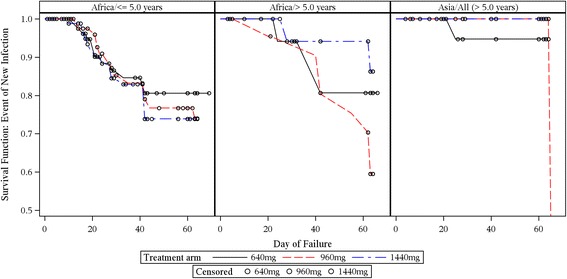
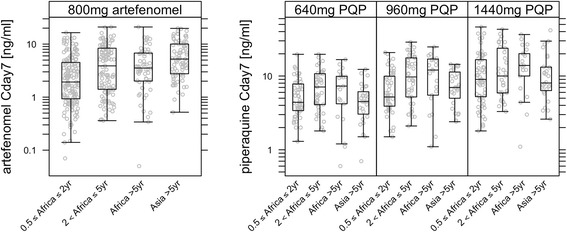
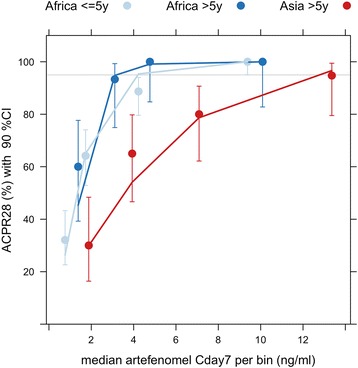
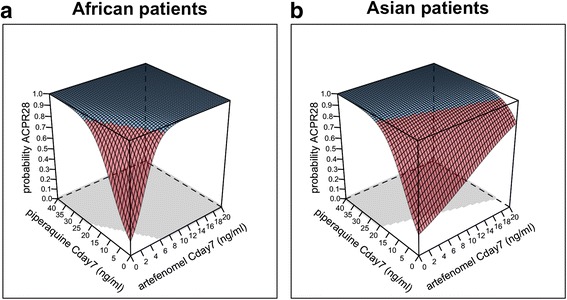
Patients in six African countries and in Vietnam were randomised to treatment with follow-up for 42-63 days. Efficacy, tolerability, safety and pharmacokinetics were assessed. Additional key objectives were to characterise the exposure-response relationship for polymerase chain reaction (PCR)-adjusted adequate clinical and parasitological response at day 28 post-dose (ACPR28) and to further investigate Kelch13 mutations. Patients in Africa (n = 355) and Vietnam (n = 82) were included, with 85% of the total population being children < 5 years of age.
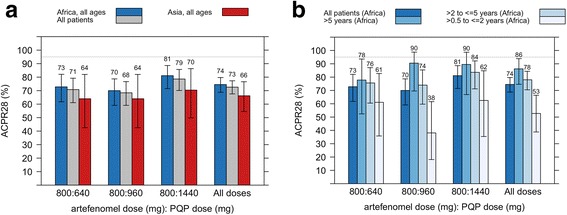
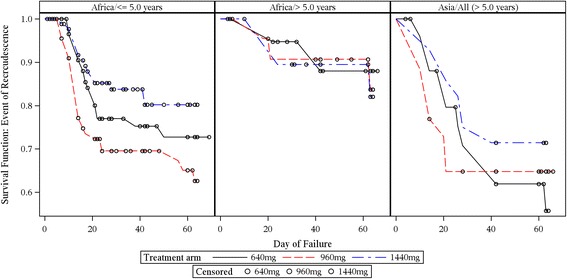
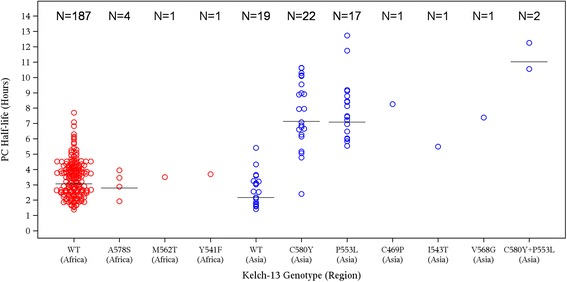
ACPR28 in the per protocol population (95% confidence interval) was 70.8% (61.13-79.19), 68.4% (59.13-76.66) and 78.6% (70.09-85.67) for doses of 800 mg artefenomel with 640 mg, 960 mg and 1440 mg of PQP respectively. ACPR28 was lower in Vietnamese than in African patients (66.2%; 54.55-76.62 and 74.5%; 68.81-79.68) respectively. Within the African population, efficacy was lowest in the youngest age group of ≥ 0.5 to ≤ 2 years, 52.7% (38.80-66.35). Initial parasite clearance was twice as long in Vietnam than in Africa. Within Vietnam, the frequency of the Kelch13 mutation was 70.1% and was clearly associated with parasite clearance half-life (PCt1/2). The most significant tolerability finding was vomiting (28.8%).
In this first clinical trial evaluating a single encounter antimalarial therapy, none of the treatment arms reached the target efficacy of > 95% PCR-adjusted ACPR at day 28. Achieving very high efficacy following single dose treatment is challenging, since > 95% of the population must have sufficient concentrations to achieve cure across a range of parasite sensitivities and baseline parasitaemia levels. While challenging, the development of tools suitable for deployment as single encounter curative treatments for adults and children in Africa and to support elimination strategies remains a key development goal.
ClinicalTrials.gov, NCT02083380 . Registered on 7 March 2014.
针对单纯性疟疾的单次治疗的临床开发有可能显著提高抗疟药的疗效。探索性数据表明,青蒿甲醚和磷酸哌喹(PQP)联合使用有可能作为单剂量疗法实现令人满意的治愈率。该研究的主要目的是确定单剂量青蒿甲醚(800毫克)加递增剂量的PQP对非洲≤5岁儿童的“目标”人群以及所有年龄段的亚洲患者中的单纯性恶性疟原虫疟疾是否为有效治疗方法。
来自六个非洲国家和越南的患者被随机分组接受治疗,并随访42至63天。评估了疗效、耐受性、安全性和药代动力学。其他关键目标是确定给药后第28天经聚合酶链反应(PCR)调整的充分临床和寄生虫学反应(ACPR28)的暴露-反应关系,并进一步研究Kelch13突变。纳入了非洲(n = 355)和越南(n = 82)的患者,总人群中85%为<5岁的儿童。
在符合方案人群中,800毫克青蒿甲醚分别与640毫克、960毫克和1440毫克PQP联合使用时,ACPR28(95%置信区间)分别为70.8%(61.13 - 79.19)、68.4%(59.13 - 76.66)和78.6%(70.09 - 85.67)。越南患者的ACPR28低于非洲患者(分别为66.2%;54.55 - 76.62和74.5%;68.81 - 79.68)。在非洲人群中,年龄最小的≥0.5至≤2岁年龄组的疗效最低,为52.7%(38.80 - 66.35)。越南的初始寄生虫清除时间是非洲的两倍。在越南,Kelch13突变的频率为70.1%,并且与寄生虫清除半衰期(PCt1/2)明显相关。最显著的耐受性发现是呕吐(28.8%)。
在这项评估单次抗疟治疗的首次临床试验中,没有一个治疗组在第28天达到经PCR调整的ACPR>95%的目标疗效。单剂量治疗后实现非常高的疗效具有挑战性,因为超过95%的人群必须有足够的浓度才能在一系列寄生虫敏感性和基线寄生虫血症水平下实现治愈。尽管具有挑战性,但开发适合在非洲作为成人和儿童单次治愈性治疗进行部署并支持消除策略的工具仍然是一个关键的发展目标。
ClinicalTrials.gov,NCT02083380。于2014年3月7日注册。