Saw Swee Hock School of Public Health, National University Health System, National University of Singapore.
Department of Infectious Diseases, Institute of Infectious Diseases and Epidemiology, Tan Tock Seng Hospital.
Clin Infect Dis. 2017 Nov 13;65(11):1905-1913. doi: 10.1093/cid/cix694.
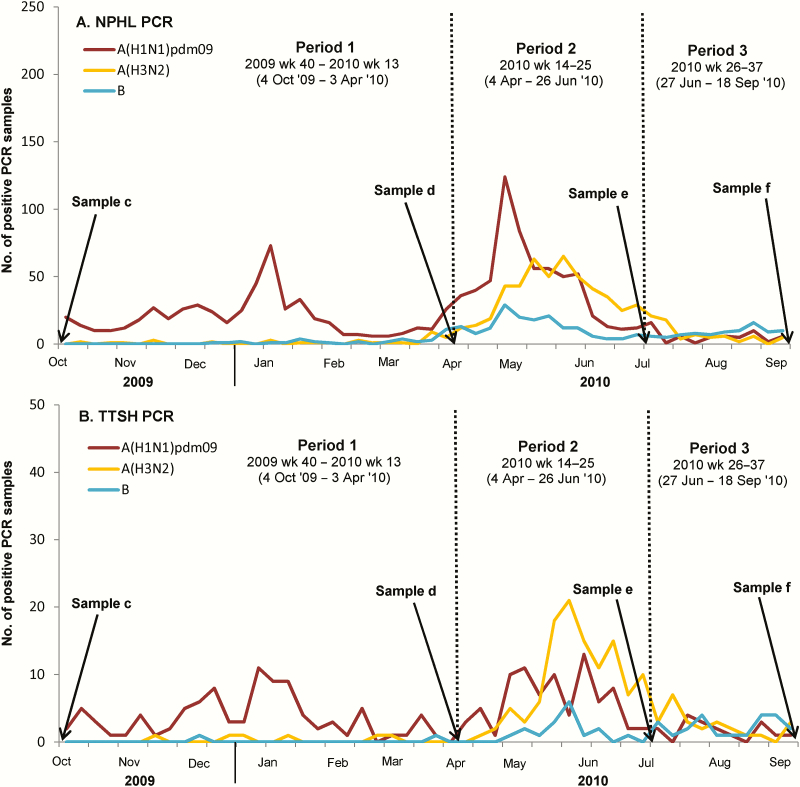
After 2009, pandemic influenza A(H1N1) [A(H1N1)pdm09] cocirculated with A(H3N2) and B in Singapore.
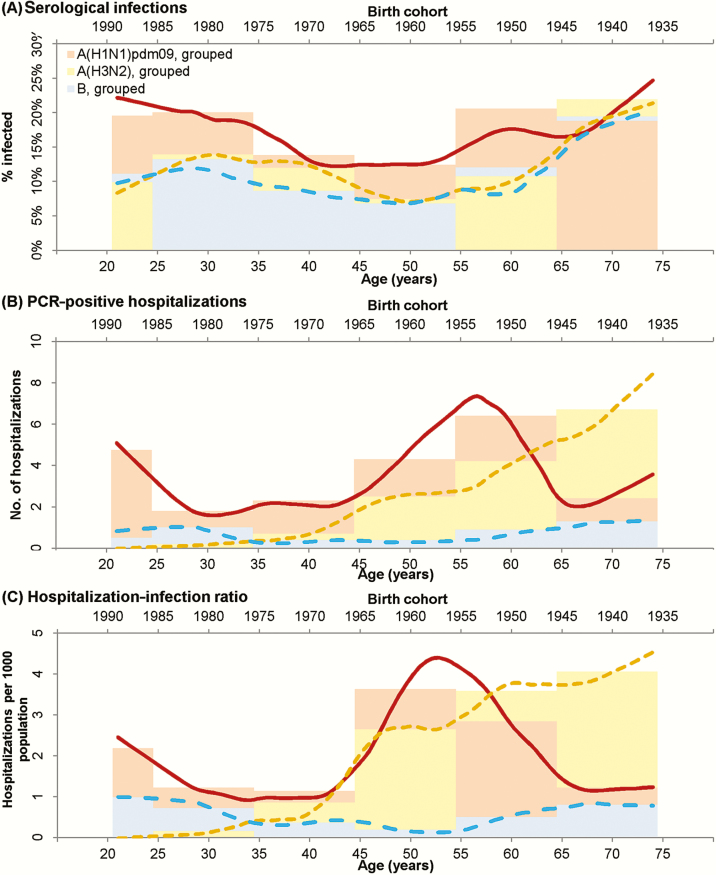
A cohort of 760 participants contributed demographic data and up to 4 blood samples each from October 2009 to September 2010. We compared epidemiology of the 3 subtypes and investigated evidence for heterotypic immunity through multivariable logistic regression using a generalized estimating equation. To examine age-related differences in severity between subtypes, we used LOESS (locally weighted smoothing) plots of hospitalization to infection ratios and explored birth cohort effects referencing the pandemic years (1957; 1968).
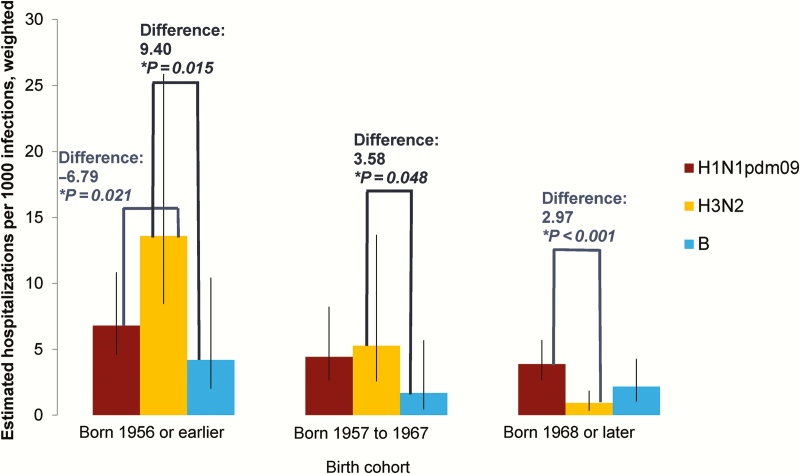
Having more household members aged 5-19 years and frequent public transport use increased risk of infection, while preexisting antibodies against the same subtype (odds ratio [OR], 0.61; P = .002) and previous influenza infection against heterotypic infections (OR, 0.32; P = .045) were protective. A(H1N1)pdm09 severity peaked in those born around 1957, while A(H3N2) severity was least in the youngest individuals and increased until it surpassed A(H1N1)pdm09 in those born in 1952 or earlier. Further analysis showed that severity of A(H1N1)pdm09 was less than that for A(H3N2) in those born in 1956 or earlier (P = .021) and vice versa for those born in 1968 or later (P < .001), with no difference in those born between 1957 and 1967 (P = .632).
Our findings suggest that childhood exposures had long-term impact on immune responses consistent with the theory of antigenic sin. This, plus observations on short-term cross-protection, have implications for vaccination and influenza epidemic and pandemic mitigation strategies.
2009 年后,甲型流感 A(H1N1)[A(H1N1)pdm09]与 A(H3N2)和 B 在新加坡共同流行。
2009 年 10 月至 2010 年 9 月期间,760 名参与者提供了人口统计学数据,并每人提供了多达 4 份血液样本。我们通过广义估计方程的多变量逻辑回归比较了这 3 种亚型的流行病学情况,并调查了异源免疫的证据。为了研究不同亚型之间严重程度的年龄相关性差异,我们使用住院与感染比值的 LOESS(局部加权平滑)图,并参考大流行年份(1957 年;1968 年)探索出生队列效应。
家中有更多年龄在 5-19 岁的成员和经常使用公共交通工具会增加感染的风险,而针对同一亚型的预先存在的抗体(比值比[OR],0.61;P =.002)和针对异源感染的先前流感感染(OR,0.32;P =.045)具有保护作用。A(H1N1)pdm09 的严重程度在大约 1957 年出生的人群中达到高峰,而 A(H3N2)的严重程度在最年轻的人群中最低,并随着年龄的增长,在 1952 年或更早出生的人群中超过 A(H1N1)pdm09。进一步的分析表明,在 1956 年或更早出生的人群中,A(H1N1)pdm09 的严重程度低于 A(H3N2)(P =.021),而在 1968 年或之后出生的人群中则相反(P <.001),在 1957 年至 1967 年之间出生的人群则没有差异(P =.632)。
我们的研究结果表明,儿童时期的暴露对免疫反应产生了长期影响,这与抗原性错误的理论一致。这一点,加上对短期交叉保护的观察,对疫苗接种和流感大流行和流行的缓解策略具有重要意义。