Murray Clare, Foden Philip, Lowe Lesley, Durrington Hannah, Custovic Adnan, Simpson Angela
Division of Infection, Immunity and Respiratory Medicine, Faculty of Biology, Medicine and Health, Manchester Academic Health Sciences Centre, University Hospital of South Manchester NHS Foundation Trust, University of Manchester, Manchester, UK; Royal Manchester Children's Hospital, Central Manchester University Hospitals NHS Foundation Trust, Manchester, UK.
Division of Infection, Immunity and Respiratory Medicine, Faculty of Biology, Medicine and Health, Manchester Academic Health Sciences Centre, University Hospital of South Manchester NHS Foundation Trust, University of Manchester, Manchester, UK.
Lancet Child Adolesc Health. 2017 Oct;1(2):114-123. doi: 10.1016/S2352-4642(17)30008-1.
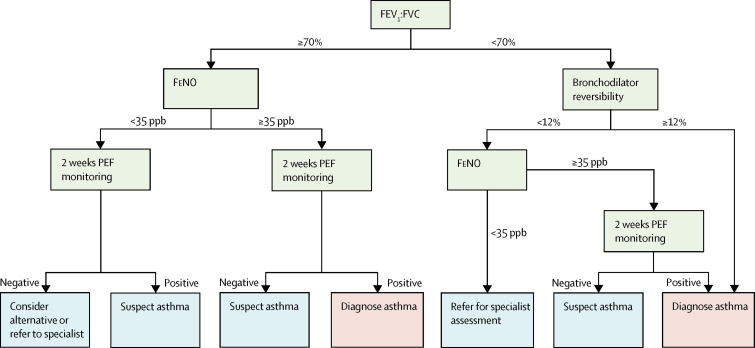
Concerns have been expressed about asthma overdiagnosis. The UK National Institute of Health and Care Excellence (NICE) proposed a new diagnostic algorithm applying four lung function measures sequentially (ratio of forced expiratory volume in 1 s [FEV] to forced vital capacity [FVC] <70%, bronchodilator reversibility ≥12%, fractional exhaled nitric oxide [FeNO] ≥35 parts per billion, and peak expiratory flow variability >20%). We aimed to assess the diagnostic value of three of the tests individually, and then test the proposed algorithm in symptomatic children.
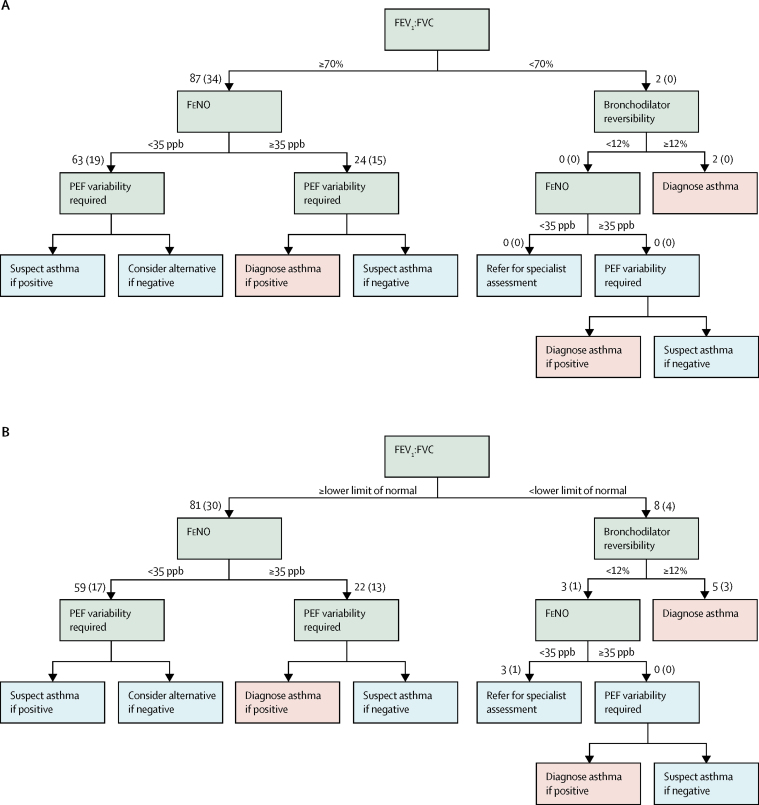
We used follow-up data at age 13-16 years from the Manchester Asthma and Allergy Study, a prospective, population-based, birth cohort study. We initially present results for the whole population, then by subgroup of disease. To simulate the situation in primary care, we included participants reporting symptoms of wheeze, cough, or breathlessness in the previous 12 months and who were not on regular inhaled corticosteroids. We used an epidemiological definition of current asthma, defined as all three of physician-diagnosed asthma, current wheeze, and current use of asthma treatment, reported by parents in a validated questionnaire. We assigned children with negative answers to all three questions as non-asthmatic controls. We also measured spirometry, bronchodilator reversibility, and FeNO at follow-up; data for peak expiratory flow variability were not available. We calculated the proportion of participants with a current positive lung function test at each step of the algorithm, and recorded the number of participants that met our definition of asthma.
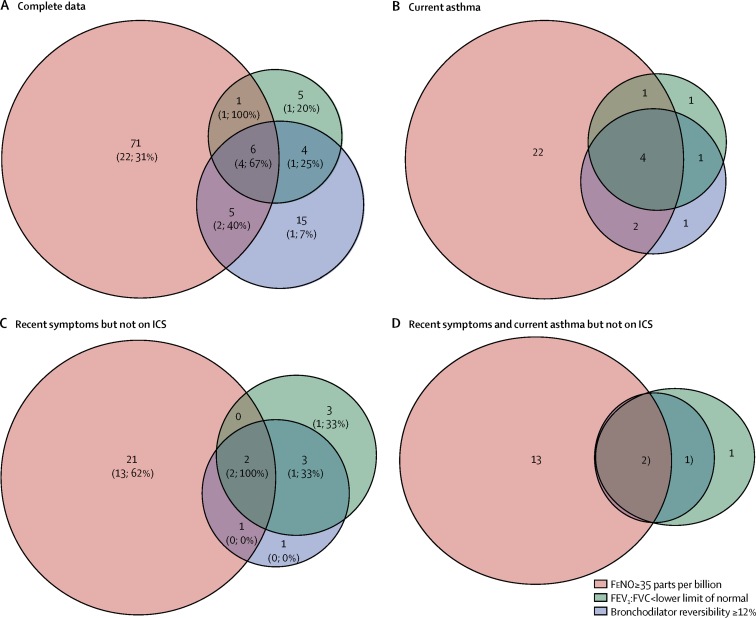
Of 1184 children born into the cohort, 772 attended follow-up at age 13-16 years between July 22, 2011, and Nov 11, 2014. Among 630 children who completed spirometry, FEV:FVC was less than 70% in ten (2%) children, of whom only two (20%) had current asthma. Bronchodilator reversibility was positive in 54 (9%) of 624 children, of whom only 12 (22%) had current asthma. FeNO was 35 or more parts per billion in 115 (24%) of 485 children, of whom 29 (25%) had current asthma. Only four of 56 children with current asthma had positive results for all three tests (spirometry, bronchodilator reversibility, and FeNO). Conversely, 24 (43%) of the 56 children with current asthma were negative on all three tests. FEV:fvc (p=0·0075) and FeNO (p<0·0001), but not bronchodilator reversibility (p=0·97), were independently associated with asthma in multivariable logistic regression models. Among children who reported recent symptoms, the diagnostic accuracy of the algorithm was poor.
Our findings challenge the proposed cutoff values for spirometry, the order in which the lung function tests are done, and the position of bronchodilator reversibility within the algorithm sequence. Until better evidence is available, the proposed NICE algorithm on asthma diagnosis should not be implemented in children.
UK Medical Research Council.
人们对哮喘的过度诊断表示担忧。英国国家卫生与临床优化研究所(NICE)提出了一种新的诊断算法,依次应用四项肺功能指标(1秒用力呼气容积[FEV]与用力肺活量[FVC]之比<70%、支气管扩张剂可逆性≥12%、呼出一氧化氮分数[FeNO]≥35 ppb以及呼气峰值流速变异性>20%)。我们旨在评估其中三项测试各自的诊断价值,然后在有症状的儿童中测试该提议的算法。
我们使用了曼彻斯特哮喘与过敏研究的13至16岁的随访数据,这是一项基于人群的前瞻性出生队列研究。我们首先展示整个人群的结果,然后按疾病亚组展示。为模拟初级保健中的情况,我们纳入了在过去12个月内报告有喘息、咳嗽或呼吸急促症状且未规律吸入糖皮质激素的参与者。我们采用当前哮喘的流行病学定义,即父母在一份经过验证的问卷中报告的医生诊断的哮喘、当前喘息以及当前使用哮喘治疗这三项均符合。我们将对所有三个问题回答为否的儿童指定为非哮喘对照。我们在随访时还测量了肺量计、支气管扩张剂可逆性和FeNO;呼气峰值流速变异性的数据不可用。我们计算了算法每个步骤中当前肺功能测试呈阳性的参与者比例,并记录符合我们哮喘定义的参与者数量。
在该队列中出生的1184名儿童中,772名在2011年7月22日至2014年11月11日期间接受了13至16岁的随访。在完成肺量计检查的630名儿童中,10名(2%)儿童的FEV:FVC低于70%,其中只有2名(20%)患有当前哮喘。624名儿童中有54名(9%)支气管扩张剂可逆性呈阳性,其中只有12名(22%)患有当前哮喘。485名儿童中有115名(24%)的FeNO为35 ppb或更高,其中29名(25%)患有当前哮喘。56名患有当前哮喘的儿童中只有4名在所有三项测试(肺量计、支气管扩张剂可逆性和FeNO)中呈阳性结果。相反,56名患有当前哮喘的儿童中有24名(43%)在所有三项测试中均为阴性。在多变量逻辑回归模型中,FEV:fvc(p = 0·0075)和FeNO(p<0·0001)与哮喘独立相关,但支气管扩张剂可逆性(p = 0·97)与哮喘无关。在报告近期症状的儿童中,该算法的诊断准确性较差。
我们的研究结果对提议的肺量计截断值、肺功能测试的进行顺序以及支气管扩张剂可逆性在算法序列中的位置提出了质疑。在获得更好的证据之前,提议的NICE哮喘诊断算法不应在儿童中实施。
英国医学研究理事会。