Department of Cardiology and Pneumology, University Medical Center Göttingen, Göttingen, Germany.
Department of Medical Statistics, University Medical Center Göttingen, Göttingen, Germany.
PLoS One. 2017 Oct 17;12(10):e0186387. doi: 10.1371/journal.pone.0186387. eCollection 2017.
There is evidence that the benefit of a primary prophylactic ICD therapy is not equal in all patients.
To evaluate risk factors of appropriate shocks and all- cause mortality in patients with a primary prophylactic ICD regarding contemporary studies.
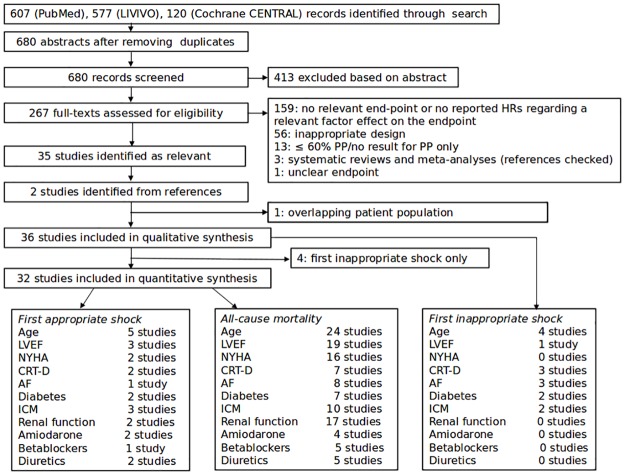
PubMed, LIVIVO, Cochrane CENTRAL between 2010 and 2016.
Studies were eligible if at least one of the endpoints of interest were reported.
All abstracts were independently reviewed by at least two authors. The full text of all selected studies was then analysed in detail.
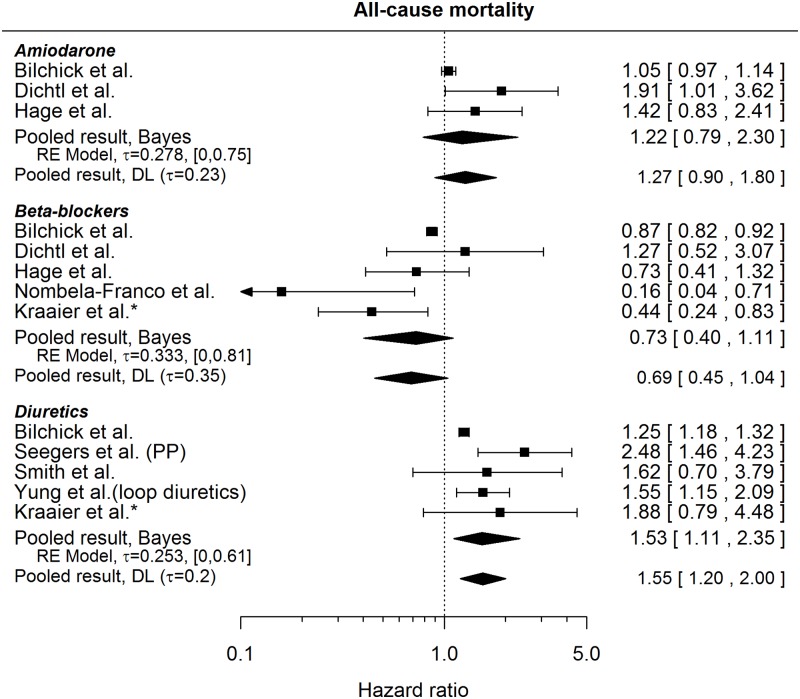
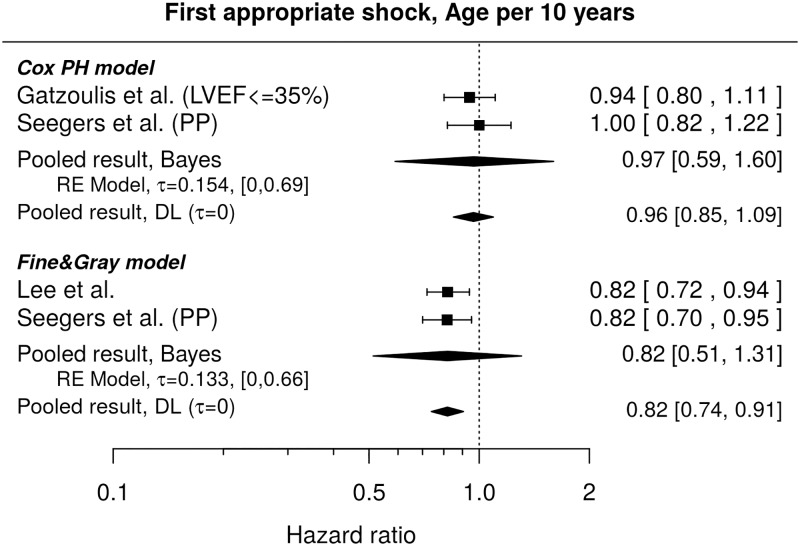
Our search strategy retrieved 608 abstracts. After exclusion of unsuitable studies, 36 papers with a total patient number of 47282 were included in our analysis. All-cause mortality was significantly associated with increasing age (HR 1.41, CI 1.29-1.53), left ventricular function (LVEF; HR 1.21, CI 1.14-1.29), ischemic cardiomyopathy (ICM; HR 1.37, CI 1.14-1.66) and co-morbidities such as impaired renal function (HR 2.30, CI 1.97-2.69). Although, younger age (HR 0.96, CI 0.85-1.09), impaired LVEF (HR 1.26, CI 0.89-1.78) and ischemic cardiomyopathy (HR 2.22, CI 0.83-5.93) were associated with a higher risk of appropriate shocks, none of these factors reached statistical significance.
Individual patient data were not available for most studies.
In this meta-analysis of contemporary clinical studies, all-cause mortality is predicted by a variety of clinical characteristics including LVEF. On the other hand, the risk of appropriate shocks might be associated with impaired LVEF and ischemic cardiomyopathy. Further prospective studies are required to verify risk factors for appropriate shocks other than LVEF to help select appropriate patients for primary prophylactic ICD-therapy.
有证据表明,初级预防性 ICD 治疗的益处并非在所有患者中均等。
评估在当代研究中,患有初级预防性 ICD 的患者中适当电击和全因死亡率的危险因素。
PubMed、LIVIVO、Cochrane CENTRAL,时间范围为 2010 年至 2016 年。
如果至少报告了一个感兴趣的终点,则研究符合条件。
所有摘要均由至少两名作者独立审查。然后详细分析所有选定研究的全文。
我们的搜索策略检索到 608 篇摘要。排除不合适的研究后,有 36 篇论文(共 47282 名患者)被纳入我们的分析。全因死亡率与年龄增加(HR 1.41,CI 1.29-1.53)、左心室功能(LVEF;HR 1.21,CI 1.14-1.29)、缺血性心肌病(ICM;HR 1.37,CI 1.14-1.66)和合并症(如肾功能受损;HR 2.30,CI 1.97-2.69)显著相关。尽管如此,年龄较轻(HR 0.96,CI 0.85-1.09)、LVEF 受损(HR 1.26,CI 0.89-1.78)和缺血性心肌病(HR 2.22,CI 0.83-5.93)与适当电击的风险增加相关,但这些因素均无统计学意义。
大多数研究都没有提供个体患者数据。
在这项当代临床研究的荟萃分析中,全因死亡率由多种临床特征预测,包括 LVEF。另一方面,适当电击的风险可能与 LVEF 受损和缺血性心肌病相关。需要进一步的前瞻性研究来验证 LVEF 以外的适当电击的危险因素,以帮助选择合适的患者进行初级预防性 ICD 治疗。