Duke Clinical Research Institute and Division of Cardiology, Duke University Medical Center, Durham, NC, USA.
Division of Cardiology, Stony Brook University, Stony Brook, NY, USA.
Eur J Heart Fail. 2018 Feb;20(2):281-291. doi: 10.1002/ejhf.1019. Epub 2017 Oct 17.
Troponin levels are commonly elevated among patients hospitalized for heart failure (HF), but the prevalence and prognostic significance of early post-discharge troponin elevation are unclear. This study sought to describe the frequency and prognostic value of pre-discharge and post-discharge troponin elevation, including persistent troponin elevation from the inpatient to outpatient settings.
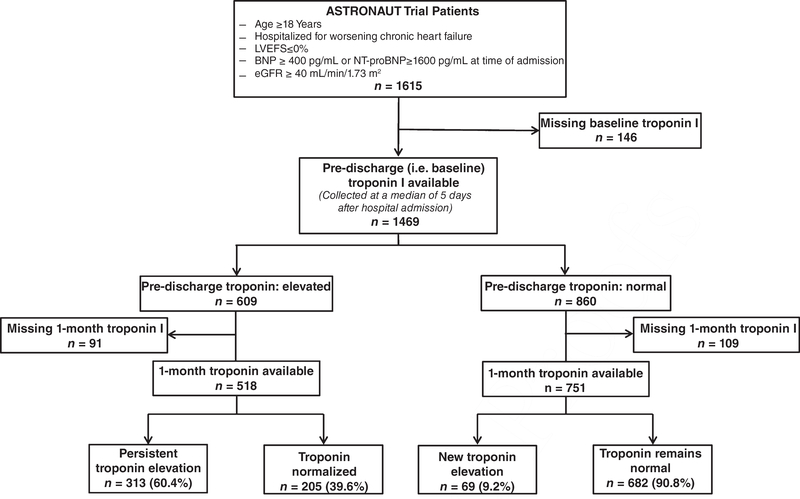
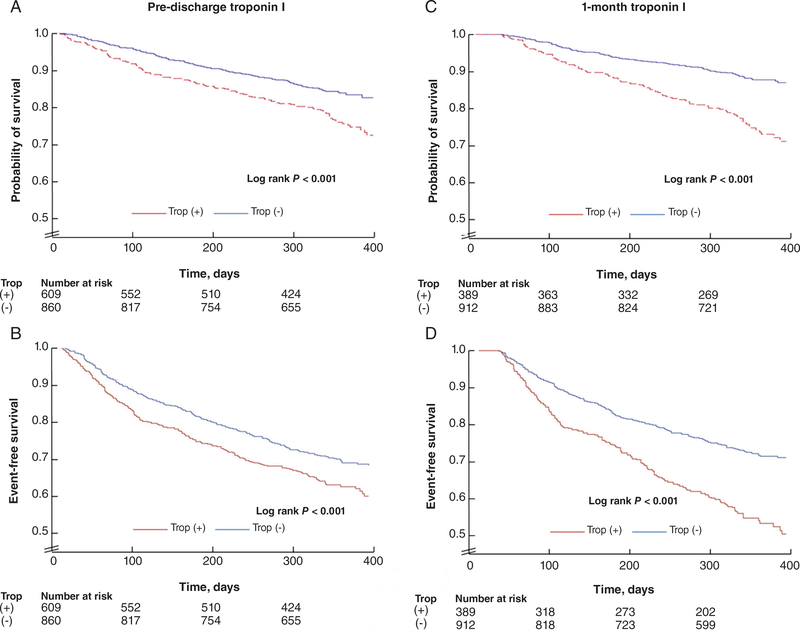
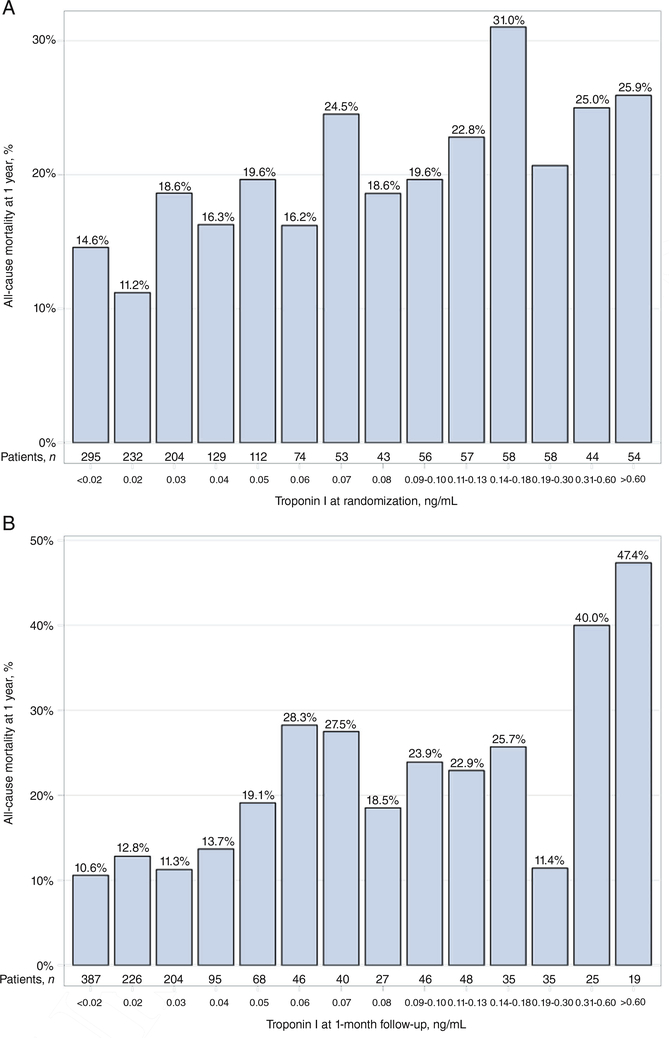
The ASTRONAUT trial (NCT00894387; http://www.clinicaltrials.gov) enrolled hospitalized HF patients with ejection fraction ≤40% and measured troponin I prior to discharge (i.e. study baseline) and at 1-month follow-up in a core laboratory (elevation defined as >0.04 ng/mL). This analysis included 1469 (91.0%) patients with pre-discharge troponin data. Overall, 41.5% and 29.9% of patients had elevated pre-discharge [median: 0.09 ng/mL; interquartile range (IQR): 0.06-0.19 ng/mL] and 1-month (median: 0.09 ng/mL; IQR: 0.06-0.15 ng/mL) troponin levels, respectively. Among patients with pre-discharge troponin elevation, 60.4% had persistent elevation at 1 month. After adjustment, pre-discharge troponin elevation was not associated with 12-month clinical outcomes. In contrast, 1-month troponin elevation was independently predictive of increased all-cause mortality [hazard ratio (HR) 1.59, 95% confidence interval (CI) 1.18-2.13] and cardiovascular mortality or HF hospitalization (HR 1.28, 95% CI 1.03-1.58) at 12 months. Associations between 1-month troponin elevation and outcomes were similar among patients with newly elevated (i.e. normal pre-discharge) and persistently elevated levels (interaction P ≥ 0.16). The prognostic value of 1-month troponin elevation for 12-month mortality was driven by a pronounced association among patients with coronary artery disease (interaction P = 0.009).
In this hospitalized HF population, troponin I elevation was common during index hospitalization and at 1-month follow-up. Elevated troponin I level at 1 month, but not pre-discharge, was independently predictive of increased clinical events at 12 months. Early post-discharge troponin I measurement may offer a practical means of risk stratification and should be investigated as a therapeutic target.
肌钙蛋白水平在因心力衰竭(HF)住院的患者中通常升高,但出院后早期肌钙蛋白升高的患病率和预后意义尚不清楚。本研究旨在描述出院前和出院后肌钙蛋白升高的频率和预后价值,包括从住院到门诊环境中持续升高的肌钙蛋白。
ASTRONAUT 试验(NCT00894387;http://www.clinicaltrials.gov)纳入了射血分数≤40%的因 HF 住院的患者,并在出院前(即研究基线)和核心实验室的 1 个月随访时测量肌钙蛋白 I(升高定义为>0.04ng/mL)。这项分析包括 1469 名(91.0%)有出院前肌钙蛋白数据的患者。总体而言,41.5%和 29.9%的患者出院前[中位数:0.09ng/mL;四分位距(IQR):0.06-0.19ng/mL]和 1 个月[中位数:0.09ng/mL;IQR:0.06-0.15ng/mL]的肌钙蛋白水平升高。在出院前肌钙蛋白升高的患者中,60.4%在 1 个月时有持续升高。调整后,出院前肌钙蛋白升高与 12 个月的临床结局无关。相比之下,1 个月时的肌钙蛋白升高独立预测全因死亡率增加[风险比(HR)1.59,95%置信区间(CI)1.18-2.13]和心血管死亡率或 HF 住院率(HR 1.28,95%CI 1.03-1.58)在 12 个月时。在新升高(即出院前正常)和持续升高水平的患者中,1 个月时肌钙蛋白升高与结局之间的相关性相似(交互 P≥0.16)。1 个月时肌钙蛋白升高对 12 个月死亡率的预后价值归因于冠心病患者中明显的相关性(交互 P=0.009)。
在该因 HF 住院的人群中,肌钙蛋白 I 在指数住院期间和 1 个月随访期间升高很常见。1 个月时升高的肌钙蛋白 I 水平,但不是出院前,与 12 个月时增加的临床事件独立相关。出院后早期测量肌钙蛋白 I 可能提供一种实用的风险分层方法,应作为治疗靶点进行研究。