Allen Stephanie M, Opondo Charles, Campbell Oona M R
Department of Population Health, Faculty of Epidemiology and Population Health, London School of Hygiene & Tropical Medicine, London, United Kingdom.
Department of Medical Statistics, Faculty of Epidemiology and Population Health, London School of Hygiene & Tropical Medicine, London, United Kingdom.
PLoS One. 2017 Oct 19;12(10):e0186515. doi: 10.1371/journal.pone.0186515. eCollection 2017.
Measurement of Emergency Obstetric Care capability is common, and measurement of newborn and overall routine childbirth care has begun in recent years. These assessments of facility capabilities can be used to identify geographic inequalities in access to functional health services and to monitor improvements over time. This paper develops an approach for monitoring the childbirth environment that accounts for the delivery caseload of the facility.
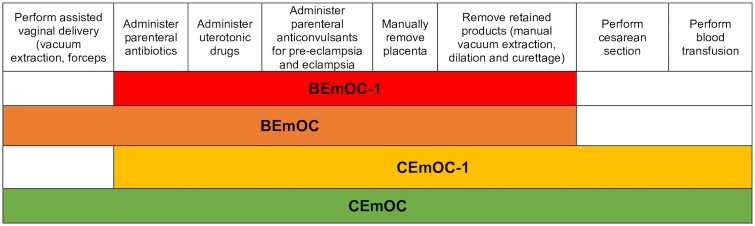
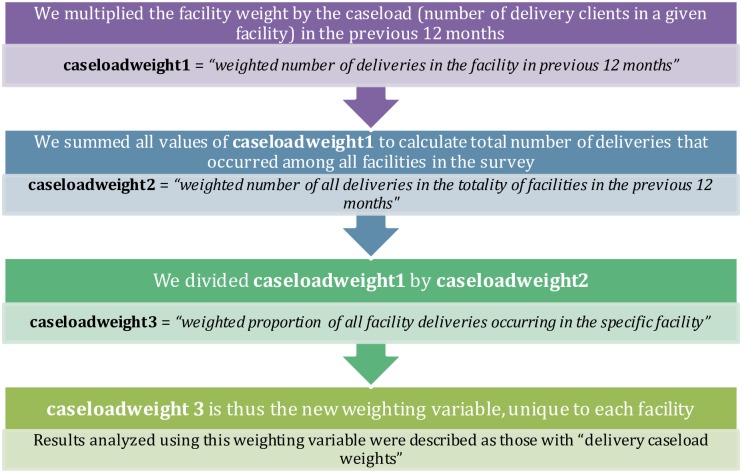
We used data from the Kenya Service Provision Assessment to examine facility capability to provide quality childbirth care, including infrastructure, routine maternal and newborn care, and emergency obstetric and newborn care. A facility was considered capable of providing a function if necessary tracer items were present and, for emergency functions, if the function had been performed in the previous three months. We weighted facility capability by delivery caseload, and compared results with those generated using traditional "survey weights".
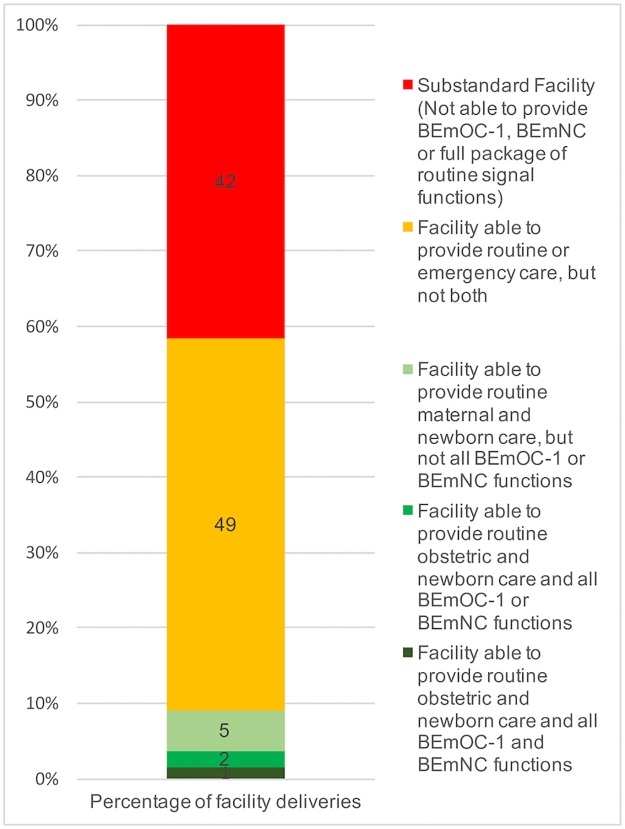
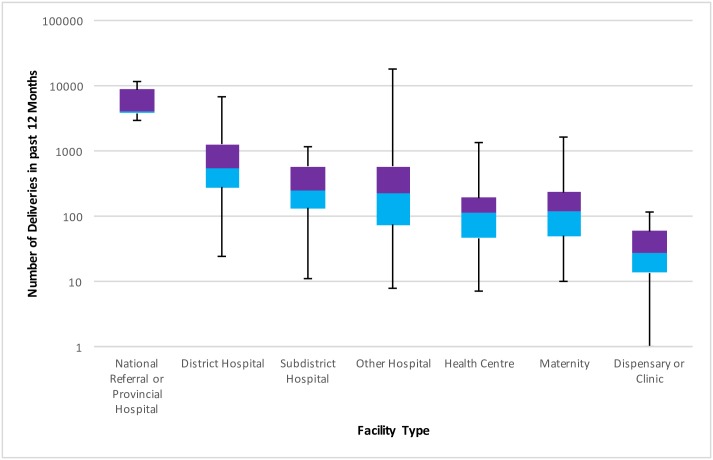
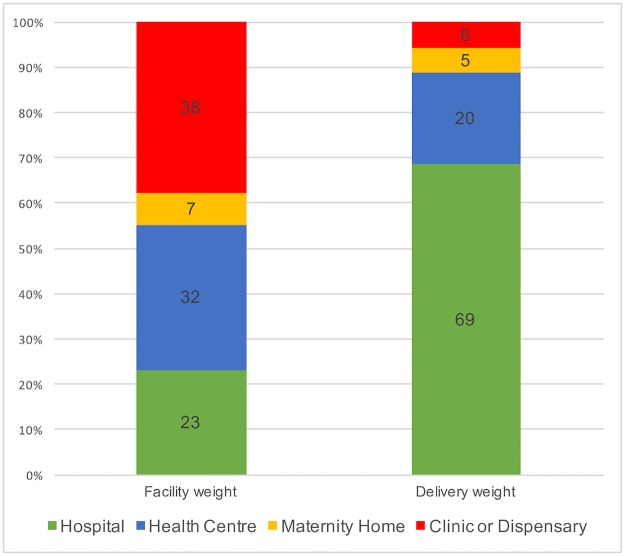
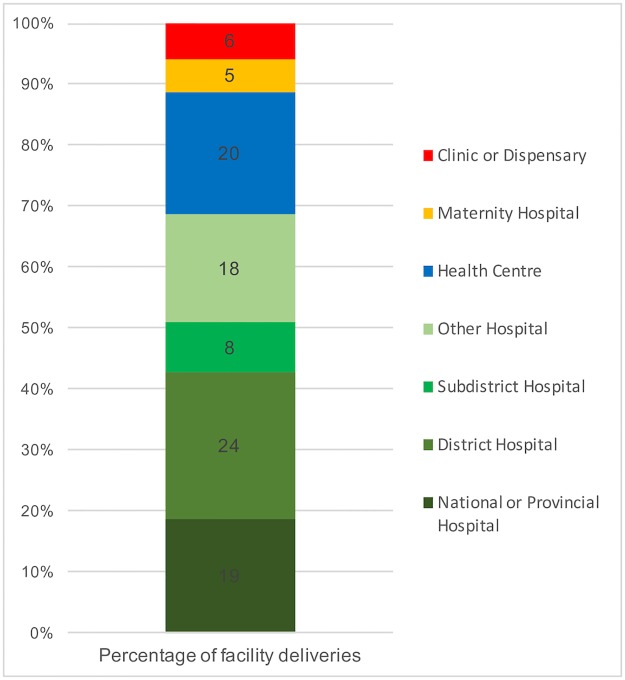
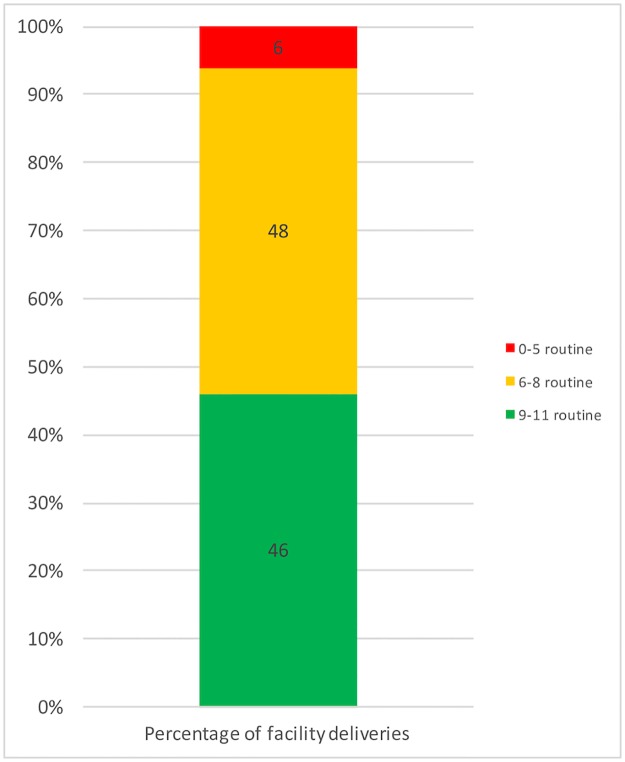
Of the 403 facilities providing childbirth care, the proportion meeting criteria for capability were: 13% for general infrastructure, 6% for basic emergency obstetric care, 3% for basic emergency newborn care, 13% and 11% for routine maternal and newborn care, respectively. When the new caseload weights accounting for delivery volume were applied, capability improved and the proportions of deliveries occurring in a facility meeting capability criteria were: 51% for general infrastructure, 46% for basic emergency obstetric care, 12% for basic emergency newborn care, 36% and 18% for routine maternal and newborn care, respectively. This is because most of the caseload was in hospitals, which generally had better capability. Despite these findings, fewer than 2% of deliveries occurred in a facility capable of providing all functions.
Reporting on the percentage of facilities capable of providing certain functions misrepresents the capacity to provide care at the national level. Delivery caseload weights allow adjustment for patient volume, and shift the denominator of measurement from facilities to individual deliveries, leading to a better representation of the context in which facility births take place. These methods could lead to more standardized national datasets, enhancing their ability to inform policy at a national and international level.
产科急诊护理能力的评估较为常见,近年来新生儿及整体常规分娩护理的评估也已展开。这些对机构能力的评估可用于识别获得功能性卫生服务方面的地理不平等,并监测随时间推移的改善情况。本文开发了一种监测分娩环境的方法,该方法考虑了机构的分娩量。
我们使用了肯尼亚服务提供评估的数据,以检查机构提供优质分娩护理的能力,包括基础设施、常规孕产妇和新生儿护理以及产科和新生儿急诊护理。如果存在必要的追踪项目,则认为该机构有能力提供某项功能;对于急诊功能,如果该功能在前三个月内已执行,则认为有能力提供。我们根据分娩量对机构能力进行加权,并将结果与使用传统“调查权重”得出的结果进行比较。
在提供分娩护理的403家机构中,达到能力标准的比例分别为:一般基础设施为13%,基本产科急诊护理为6%,基本新生儿急诊护理为3%,常规孕产妇和新生儿护理分别为13%和11%。当应用考虑分娩量的新的病例数权重时,能力有所提高,在达到能力标准的机构中发生的分娩比例分别为:一般基础设施为51%,基本产科急诊护理为46%,基本新生儿急诊护理为12%,常规孕产妇和新生儿护理分别为36%和18%。这是因为大部分分娩量集中在医院,而医院的能力通常更好。尽管有这些发现,但在能够提供所有功能的机构中进行的分娩不到2%。
报告能够提供某些功能的机构的百分比会歪曲国家层面的护理提供能力。分娩量权重允许根据患者数量进行调整,并将测量的分母从机构转移到个体分娩,从而更好地反映机构分娩发生的背景。这些方法可能会导致更标准化的国家数据集,增强其为国家和国际层面政策提供信息的能力。