Pfortmueller Carmen Andrea, Meisel Christian, Fux Michaela, Schefold Joerg C
Department of Intensive Care Medicine, Inselspital, Bern University Hospital, University of Bern, Freiburgstrasse 10, 3010, Bern, Switzerland.
Department of Medical Immunology, Charité University Hospital Berlin, Augustenburger Platz 1, 13353, Berlin, Germany.
Intensive Care Med Exp. 2017 Oct 23;5(1):49. doi: 10.1186/s40635-017-0163-0.
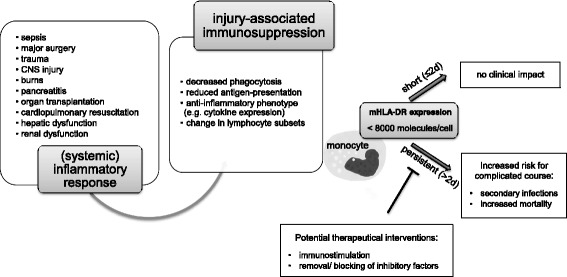
In critically ill patients, organ dysfunctions are routinely assessed, monitored, and treated. Mounting data show that substantial critical illness-induced changes in the immune system can be observed in most ICU patients and that not only "hyper-inflammation" but also persistence of an anti-inflammatory phenotype (as in sepsis-associated immunosuppression) is associated with increased morbidity and mortality. Despite common perception, changes in functional immunity cannot be adequately assessed by routine inflammatory biomarkers such as C-reactive protein, procalcitonin, or numerical analysis of leukocyte (sub)-counts. Cytokines appear also not suited due to their short half-life and pleiotropy, their unexclusive origin from immune cells, and their potential to undergo antagonization by circulating inactivating molecules. Thus, beyond leukocyte quantification and use of routine biomarkers, direct assessment of immune cell function seems required to characterize the immune systems' status. This may include determination of, e.g., ex vivo cellular cytokine release, phagocytosis activity, and/or antigen-presenting capacity. In this regard, standardized flow-cytometric assessment of the major histocompatibility-II complex human leukocyte antigen (-D related) (HLA-DR) has gained particular interest. Monocytic HLA-DR (mHLA-DR) controls the interplay between innate and adaptive immunity and may serve as a "global" biomarker of injury-associated immunosuppression, and its decreased expression is associated with adverse clinical outcomes (e.g., secondary infection risk, mortality). Importantly, recent data demonstrate that injury-associated immunosuppression can be reversed-opening up new therapeutic avenues in affected patients. Here we discuss the potential scientific and clinical value of assessment of functional immunity with a focus on monocytes/macrophages and review the current state of knowledge and potential perspectives for affected critically ill patients.
在危重症患者中,器官功能障碍会定期进行评估、监测和治疗。越来越多的数据表明,在大多数重症监护病房(ICU)患者中都能观察到严重疾病引起的免疫系统显著变化,而且不仅“过度炎症反应”,抗炎症表型的持续存在(如脓毒症相关免疫抑制)也与发病率和死亡率增加有关。尽管普遍认为,常规炎症生物标志物如C反应蛋白、降钙素原或白细胞(亚群)计数的数值分析无法充分评估功能性免疫的变化。细胞因子似乎也不合适,因为它们半衰期短且具有多效性,并非仅由免疫细胞产生,且可能会被循环中的失活分子拮抗。因此,除了白细胞定量和使用常规生物标志物外,似乎还需要直接评估免疫细胞功能来表征免疫系统的状态。这可能包括例如测定体外细胞因子释放、吞噬活性和/或抗原呈递能力。在这方面,对主要组织相容性复合体-II类人类白细胞抗原(-D相关)(HLA-DR)进行标准化流式细胞术评估引起了特别关注。单核细胞HLA-DR(mHLA-DR)控制着先天性免疫和适应性免疫之间的相互作用,可作为损伤相关免疫抑制的“整体”生物标志物,其表达降低与不良临床结局(如继发感染风险、死亡率)相关。重要的是,最近的数据表明,损伤相关免疫抑制可以逆转,为受影响的患者开辟了新的治疗途径。在此,我们讨论评估功能性免疫的潜在科学和临床价值,重点关注单核细胞/巨噬细胞,并回顾受影响的危重症患者的当前知识状态和潜在前景。