The George Institute for Global Health, University of Sydney, Camperdown, Australia
The George Institute for Global Health, University of Sydney, Camperdown, Australia.
J Am Heart Assoc. 2017 Oct 24;6(10):e007093. doi: 10.1161/JAHA.117.007093.
We evaluated a multifaceted, computerized quality improvement intervention for management of cardiovascular disease (CVD) risk in Australian primary health care. After completion of a cluster randomized controlled trial, the intervention was made available to both trial arms. Our objective was to assess intervention outcomes in the post-trial period and any heterogeneity based on original intervention allocation.
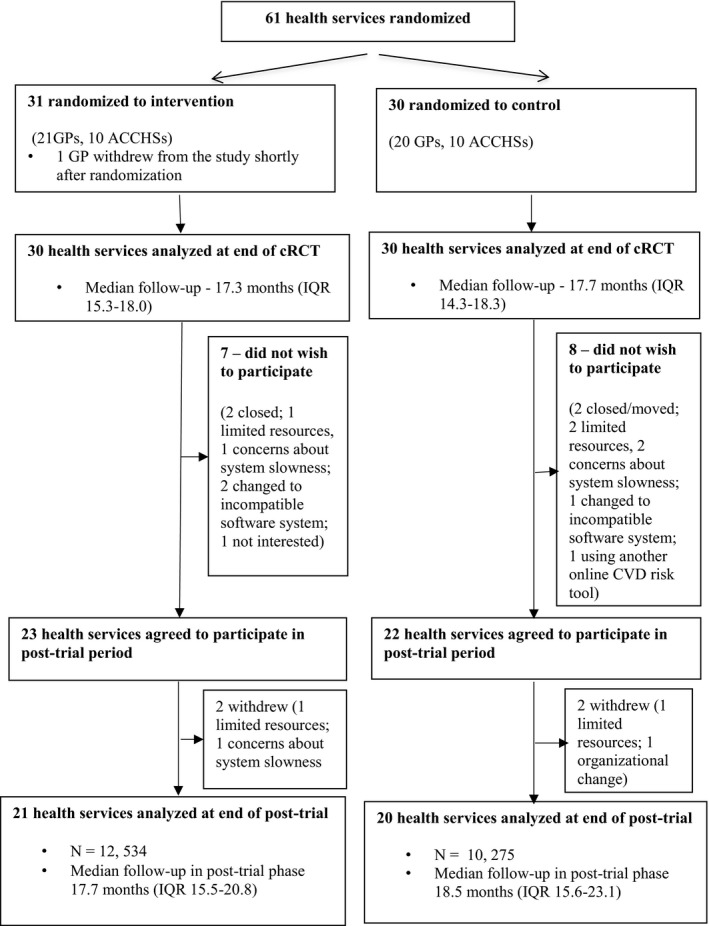
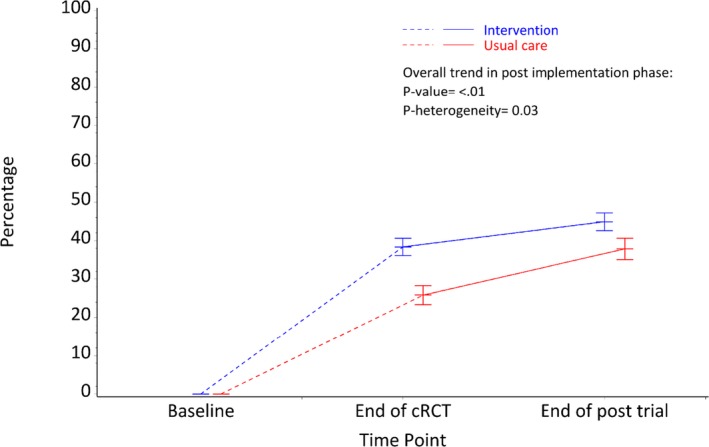
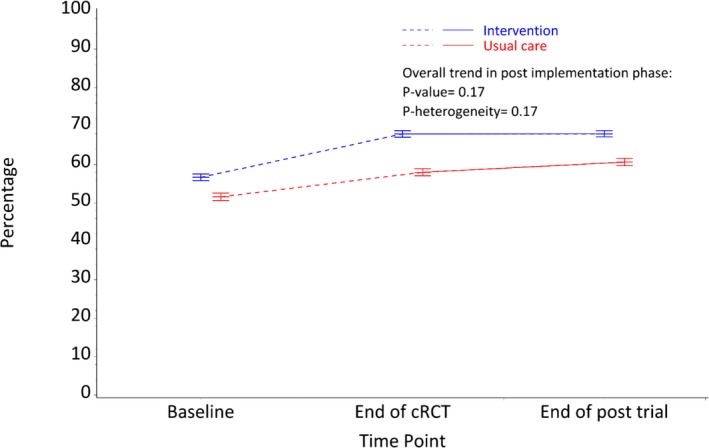
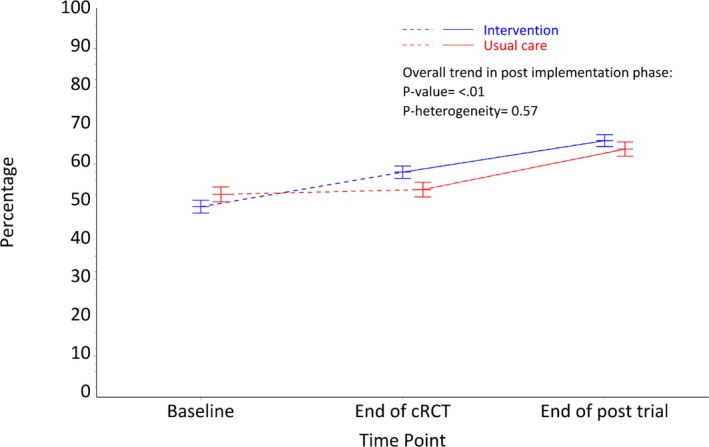
Data from 41 health services were analyzed. Outcomes were (1) proportion of eligible population with guideline-recommended CVD risk factor measurements; and (2) the proportion at high CVD risk with current prescriptions for guideline-recommended medications. Patient-level analyses were conducted using generalized estimating equations to account for clustering and time effects and tests for heterogeneity were conducted to assess impact of original treatment allocation. Median follow-up for 22 809 patients (mean age, 64.2 years; 42.5% men, 26.5% high CVD risk) was 17.9 months post-trial and 35 months since trial inception. At the end of the post-trial period there was no change in CVD risk factor screening overall when compared with the end of the trial period (64.7% versus 63.5%, =0.17). For patients at high CVD risk, there were significant improvements in recommended prescriptions at end of the post-trial period when compared with the end of the trial period (65.2% versus 56.0%, <0.001). There was no heterogeneity of treatment effects on the outcomes based on original randomization allocation.
CVD risk screening improvements were not observed in the post-trial period. Conversely, improvements in prescribing continued, suggesting that changes in provider and patient actions may take time when initiating medications.
URL: http://www.anzctr.org.au. Unique identifier: 12611000478910.
我们评估了一种多方面的、计算机化的质量改进干预措施,以管理澳大利亚初级医疗保健中的心血管疾病(CVD)风险。在完成一项集群随机对照试验后,该干预措施可供试验组使用。我们的目的是评估试验后期间的干预结果,以及基于原始干预分配的任何异质性。
分析了 41 个卫生服务的数据。结果为:(1)符合指南建议的 CVD 危险因素测量标准的合格人群比例;(2)目前有指南推荐药物处方的高危 CVD 人群比例。使用广义估计方程对患者水平进行分析,以考虑聚类和时间效应,并进行异质性检验,以评估原始治疗分配的影响。对 22809 名患者(平均年龄 64.2 岁;男性 42.5%,高危 CVD 26.5%)进行了中位随访 17.9 个月(试验结束后)和 35 个月(试验开始后)。与试验结束时相比,在试验结束后期间,CVD 危险因素筛查总体上没有变化(64.7%比 63.5%,=0.17)。对于高危 CVD 的患者,与试验结束时相比,试验结束后推荐处方有显著改善(65.2%比 56.0%,<0.001)。基于原始随机分组分配,治疗效果没有异质性。
在试验后期间没有观察到 CVD 风险筛查的改善。相反,处方的改善仍在继续,这表明在开始使用药物时,提供者和患者的行为改变可能需要时间。