Department of Surgery, University of Virginia, 1215 Lee Street, Charlottesville, VA, 22903, USA.
Surg Endosc. 2018 Apr;32(4):2131-2136. doi: 10.1007/s00464-017-5911-4. Epub 2017 Oct 24.
The number of robotic surgical procedures performed yearly is constantly rising, due to improved dexterity and visualization capabilities compared with conventional methods. We hypothesized that outcomes after robotic-assisted inguinal hernia repair would not be significantly different from outcomes after laparoscopic or open repair.
All patients undergoing inguinal hernia repair between 2012 and 2016 were identified using institutional American College of Surgeons National Surgical Quality Improvement Program data. Demographics; preoperative, intraoperative, and postoperative characteristics; and outcomes were evaluated based on method of repair (Robot, Lap, or Open). Categorical variables were analyzed by Chi-square test and continuous variables using Mann-Whitney U.
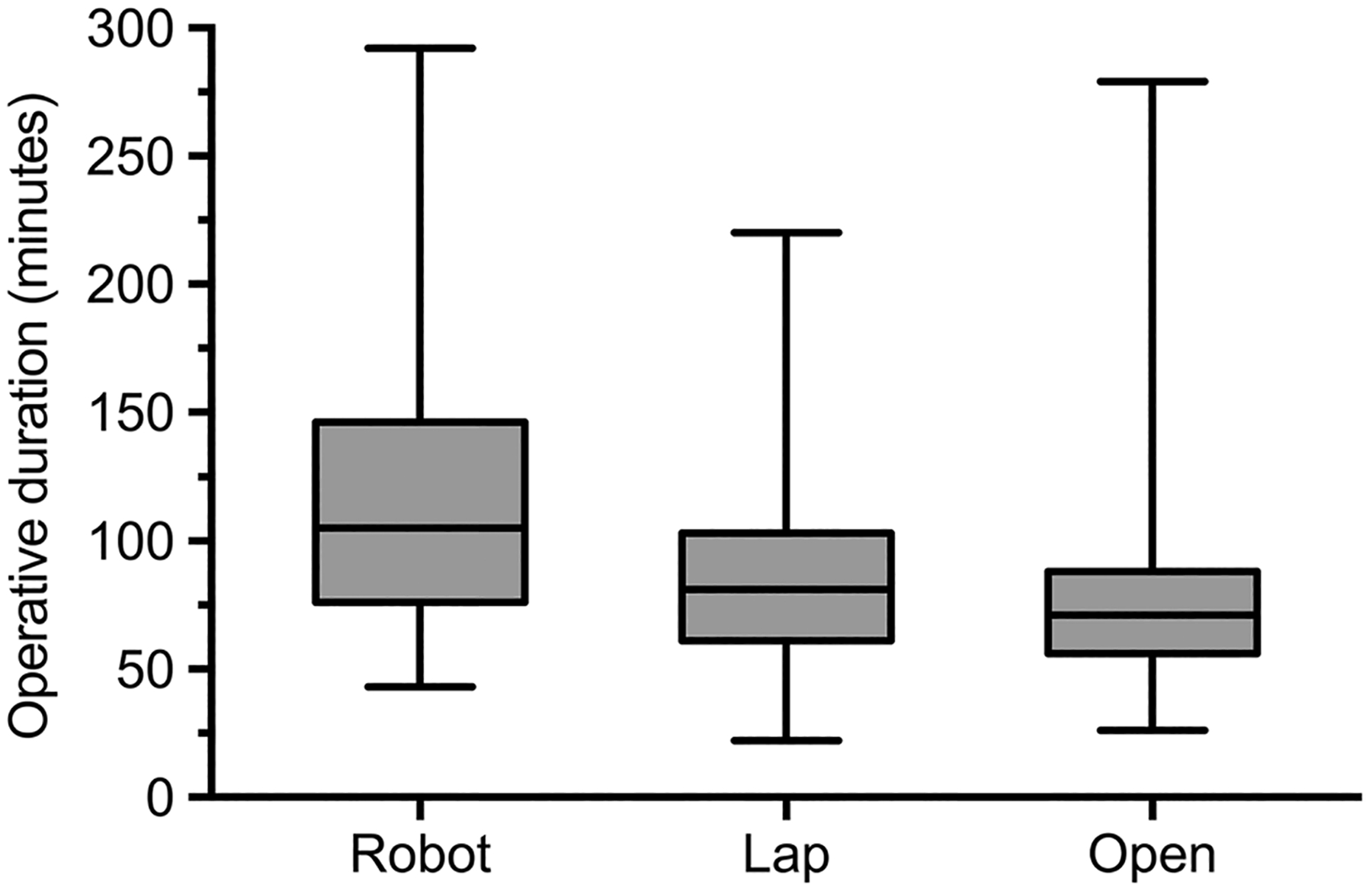
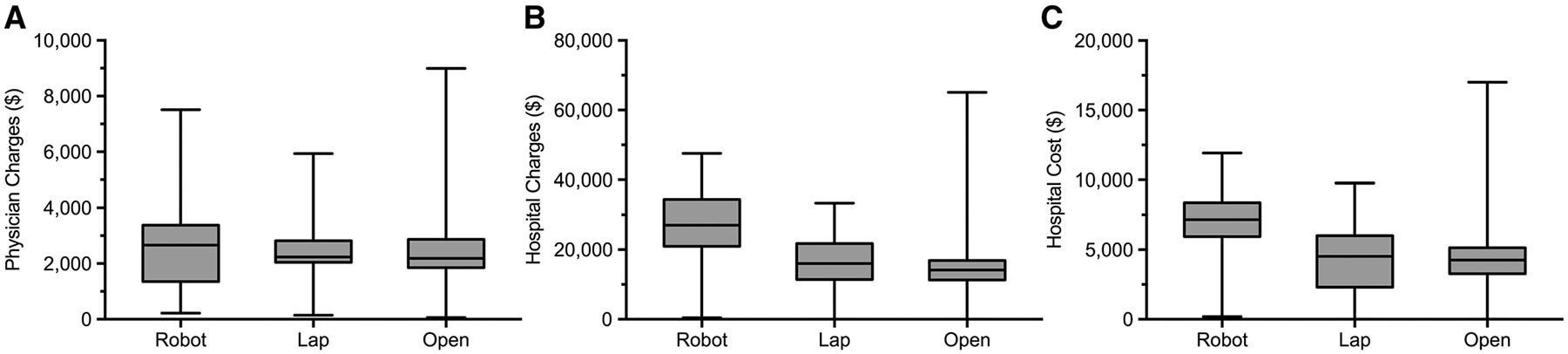
A total of 510 patients were identified who underwent unilateral inguinal hernia repair (Robot: 13.8% [n = 69], Lap: 48.1% [n = 241], Open: 38.1% [n = 191]). There were no demographic differences between groups other than age (Robot: 52 [39-62], Lap: 57 [45-67], and Open: 56 [48-67] years, p = 0.03). Operative duration was also different (Robot: 105 [76-146] vs. Lap: 81 [61-103] vs. Open: 71 [56-88] min, p < 0.001). There were no operative mortalities and all patients except one were discharged home the same day. Postoperative occurrences (adverse events, readmissions, and death) were similar between groups (Robot: 2.9% [2], Lap: 3.3% [8], Open: 5.2% [10], p = 0.53). Although rare, there was a significant difference in rate of postoperative skin and soft tissue infection (Robot: 2.9% [2] vs. Lap: 0% [0] vs. Open: 0.5% [1], p = 0.02). Cost was significantly different between groups (Robot: $7162 [$5942-8375] vs. Lap: $4527 [$2310-6003] vs. Open: $4264 [$3277-5143], p < 0.001).
Outcomes after robotic-assisted inguinal hernia repair were similar to outcomes after laparoscopic or open repair. Longer operative duration during robotic repair may contribute to higher rates of skin and soft tissue infection. Higher cost should be considered, along with surgeon comfort level and patient preference when deciding whether inguinal hernia repair is approached robotically.
与传统方法相比,机器人手术具有更高的灵活性和可视化能力,因此每年进行的机器人手术数量不断增加。我们假设机器人辅助腹股沟疝修补术的结果不会与腹腔镜或开放修补术的结果有显著差异。
使用机构美国外科医师学会国家手术质量改进计划数据确定 2012 年至 2016 年间接受腹股沟疝修补术的所有患者。根据修补方法(机器人、腹腔镜或开放)评估人口统计学;术前、术中、术后特征;和结果。分类变量采用卡方检验分析,连续变量采用曼-惠特尼 U 检验。
共确定了 510 例单侧腹股沟疝修补术患者(机器人:13.8%[n=69],腹腔镜:48.1%[n=241],开放:38.1%[n=191])。除年龄外,各组之间没有其他差异(机器人:52[39-62],腹腔镜:57[45-67],开放:56[48-67]岁,p=0.03)。手术时间也不同(机器人:105[76-146]vs.腹腔镜:81[61-103]vs.开放:71[56-88]分钟,p<0.001)。没有手术死亡,除 1 例患者外,所有患者均于当天出院回家。术后并发症(不良事件、再入院和死亡)在各组之间相似(机器人:2.9%[2],腹腔镜:3.3%[8],开放:5.2%[10],p=0.53)。尽管罕见,但术后皮肤和软组织感染的发生率存在显著差异(机器人:2.9%[2]vs.腹腔镜:0%[0]vs.开放:0.5%[1],p=0.02)。各组之间的费用差异显著(机器人:7162[5942-8375]美元vs.腹腔镜:4527[2310-6003]美元vs.开放:4264[3277-5143]美元,p<0.001)。
机器人辅助腹股沟疝修补术的结果与腹腔镜或开放修补术的结果相似。机器人修复过程中较长的手术时间可能导致皮肤和软组织感染的发生率增加。在决定是否采用机器人进行腹股沟疝修补术时,应考虑更高的成本,以及外科医生的舒适度和患者的偏好。