Department of Social Medicine, School of Public Health, Fudan University, P.O.Box 250, 138 Yi Xue Yuan Road, Shanghai, 200032, China.
Key Lab of Health Technology Assessment, National Health and Family Planning Commission of the People's Republic of China, Fudan University, Shanghai, 200032, China.
Int J Equity Health. 2017 Oct 25;16(1):185. doi: 10.1186/s12939-017-0686-8.
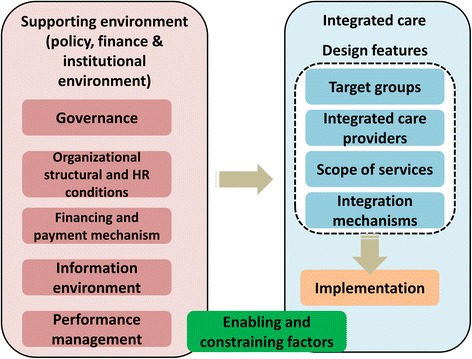
Initiatives on integrated care between hospitals and community health centers (CHCs) have been introduced to transform the current fragmented health care delivery system into an integrated system in China. Up to date no research has analyzed in-depth the experiences of these initiatives based on perspectives from various stakeholders. This study analyzed the integrated care pilot in Hangzhou City by investigating stakeholders' perspectives on its design features and supporting environment, their acceptability of this pilot, and further identifying the enabling and constraining factors that may influence the implementation of the integrated care reform.
The qualitative study was carried out based on in-depth interviews and focus group discussions with 50 key informants who were involved in the policy-making process and implementation. Relevant policy documents were also collected for analysis.
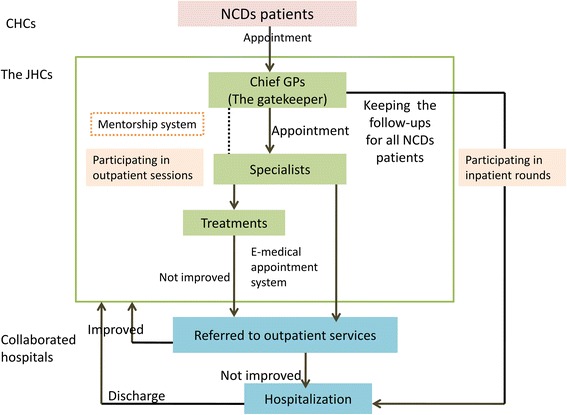
The pilot in Hangzhou was established as a CHC-led delivery system based on cooperation agreement between CHCs and hospitals to deliver primary and specialty care together for patients with chronic diseases. An innovative learning-from-practice mentorship system between specialists and general practitioners was also introduced to solve the poor capacity of general practitioners. The design of the pilot, its governance and organizational structure and human resources were enabling factors, which facilitated the integrated care reform. However, the main constraining factors were a lack of an integrated payment mechanism from health insurance and a lack of tailored information system to ensure its sustainability.
The integrated care pilot in Hangzhou enabled CHCs to play as gate-keeper and care coordinator for the full continuum of services across the health care providers. The government put integrated care a priority, and constructed an efficient design, governance and organizational structure to enable its implementation. Health insurance should play a proactive role, and adopt a shared financial incentive system to support integrated care across providers in the future.
为了将当前碎片化的医疗服务体系转变为整合体系,中国已经推出了医院与社区卫生服务中心(CHC)之间的综合关怀举措。迄今为止,尚无研究从各个利益相关者的角度深入分析这些举措的经验。本研究通过调查利益相关者对试点的设计特点和支持环境、对该试点的接受程度,以及进一步确定可能影响综合关怀改革实施的有利和制约因素,分析了杭州市的综合关怀试点。
本定性研究基于对 50 名关键知情者的深入访谈和焦点小组讨论,这些知情者参与了政策制定过程和实施。还收集了相关政策文件进行分析。
杭州的试点是以 CHC 为主导的交付系统,基于 CHC 和医院之间的合作协议,共同为慢性病患者提供初级和专科护理。还引入了专科医生和全科医生之间的创新实践指导师制度,以解决全科医生能力不足的问题。试点的设计、治理和组织结构以及人力资源是有利因素,促进了综合关怀改革。然而,主要的制约因素是医疗保险缺乏整合支付机制和缺乏定制化信息系统来确保其可持续性。
杭州的综合关怀试点使 CHC 能够充当医疗服务提供者全流程服务的守门人和协调者。政府将综合关怀作为优先事项,并构建了高效的设计、治理和组织结构,以支持其实施。医疗保险应发挥积极作用,采用共享财务激励制度,以支持未来医疗服务提供者之间的综合关怀。