Anand Shuchi, Zheng Yuanchao, Montez-Rath Maria E, Wei Wang Jin, Perico Norberto, Carminati Sergio, Narayan Km Venkat, Tandon Nikhil, Mohan Viswanathan, Jha Vivekanand, Zhang Luxia, Remuzzi Giuseppe, Prabahkaran Dorairaj, Chertow Glenn M
Division of Nephrology, Stanford University School of Medicine, Stanford, California, USA.
Renal Division, Department of Medicine, Peking University First Hospital, Beijing, China.
BMJ Glob Health. 2017 Oct 9;2(4):e000453. doi: 10.1136/bmjgh-2017-000453. eCollection 2017.
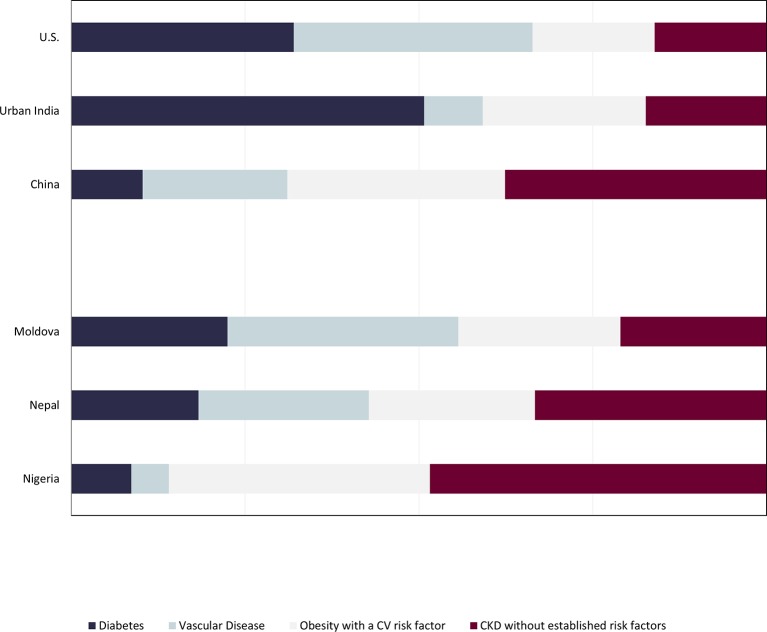
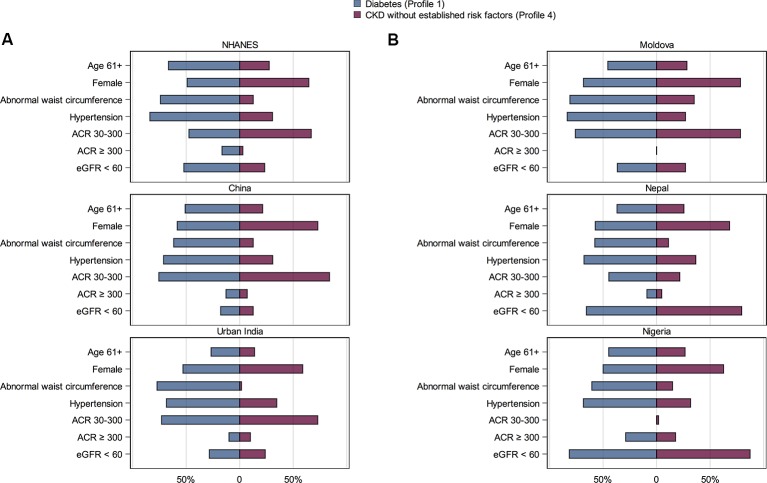
Kidney biopsies to elucidate the cause of chronic kidney disease (CKD) are performed in a minority of persons with CKD living in high-income countries, since associated conditions-that is, diabetes mellitus, vascular disease or obesity with pre-diabetes, prehypertension or dyslipidaemia-can inform management targeted at slowing CKD progression in a majority. However, attributes of CKD may differ substantially among persons living in low-income and middle-income countries (LMICs). We used data from population or community-based studies from five LMICs (China, urban India, Moldova, Nepal and Nigeria) to determine what proportion of persons with CKD living in diverse regions fit one of the three major clinical profiles, with data from the US National Health Nutrition and Examination Survey as reference. In the USA, urban India and Moldova, 79.0%-83.9%; in China and Nepal, 62.4%-66.7% and in Nigeria, 51.6% persons with CKD fit one of three established risk profiles. Diabetes was most common in urban India and vascular disease in Moldova (50.7% and 33.2% of persons with CKD in urban India and Moldova, respectively). In Nigeria, 17.8% of persons with CKD without established risk factors had albuminuria ≥300 mg/g, the highest proportion in any country. While the majority of persons with CKD in LMICs fit into one of three established risk profiles, the proportion of persons who have CKD without established risk factors is higher than in the USA. These findings can inform tailored CKD detection and management systems and highlight the importance of studying potential causes and outcomes of CKD without established risk factors in LMICs.
在高收入国家,只有少数慢性肾脏病(CKD)患者会进行肾活检以明确病因,因为相关疾病,即糖尿病、血管疾病或伴有糖尿病前期、高血压前期或血脂异常的肥胖症,能够为大多数旨在延缓CKD进展的管理提供依据。然而,低收入和中等收入国家(LMICs)的CKD患者的特征可能有很大差异。我们使用了来自五个LMICs(中国、印度城市地区、摩尔多瓦、尼泊尔和尼日利亚)基于人群或社区的研究数据,以确定生活在不同地区的CKD患者中符合三种主要临床特征之一的比例,并将美国国家健康与营养检查调查的数据作为参考。在美国、印度城市地区和摩尔多瓦,79.0%-83.9%的CKD患者符合三种既定风险特征之一;在中国和尼泊尔,这一比例为62.4%-66.7%;在尼日利亚,这一比例为51.6%。糖尿病在印度城市地区最为常见,血管疾病在摩尔多瓦最为常见(分别占印度城市地区和摩尔多瓦CKD患者的50.7%和33.2%)。在尼日利亚,17.8%无既定风险因素的CKD患者蛋白尿≥300mg/g,这一比例在所有国家中最高。虽然大多数LMICs的CKD患者符合三种既定风险特征之一,但无既定风险因素的CKD患者比例高于美国。这些发现可为量身定制的CKD检测和管理系统提供参考,并突出了研究LMICs中无既定风险因素的CKD潜在病因和结局的重要性。