De Jong Cornelis N, Saes Lotte, Klerk Clara P W, Van der Klift Marjolein, Cornelissen Jan J, Broers Annoek E C
Department of Hematology, Erasmus Medical Center, Rotterdam, the Netherlands.
Department of Hematology and Oncology, Onze Lieve Vrouwe Gasthuis, Amsterdam, the Netherlands.
PLoS One. 2017 Oct 26;12(10):e0187184. doi: 10.1371/journal.pone.0187184. eCollection 2017.
Acute graft-versus-host disease (aGVHD) is an important complication of allogeneic stem cell transplantation (alloSCT). High dose glucocorticosteroids, are currently recommended as first-line treatment for grade II-IV aGVHD resulting in overall complete responses (CR) in 40%-50% of patients. No standard second-line regimen has been established. Different options have been reported, including anti-TNFα antibodies.
We retrospectively reviewed the outcome of 15 patients with steroid-refractory (SR) aGVHD treated with etanercept at our institution. Patients were transplanted for a hematological malignancy and received either a myeloablative or a non-myeloablative conditioning regimen. Prophylaxis of GVHD consisted of cyclosporin A and mycophenolic acid.
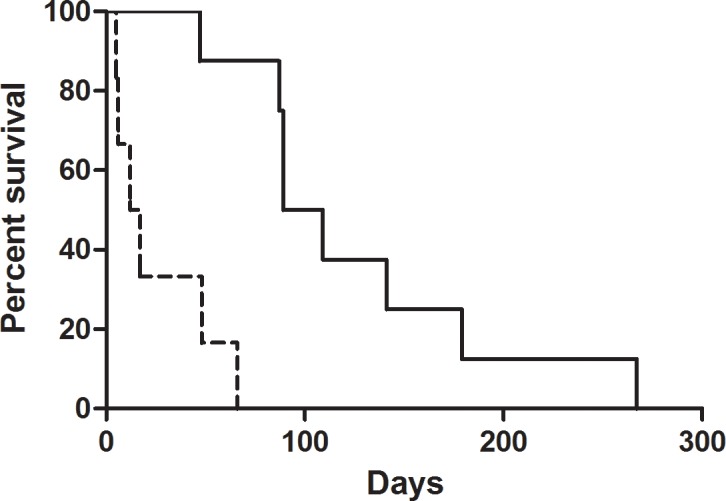
Acute GVHD was diagnosed at a median of 61 days post-transplantation. All patients had grade III aGVHD of the gut. Second-line treatment with etanercept was started at a median of 13 days after initiation of first-line therapy. Overall response rate was 53%, with CR in 3 patients and PR in 5 patients. Median overall survival after initiation of treatment with etanercept was 66 days (range 5-267) for the entire group. Median overall survival was 99 days (range 47-267 days) for responders and 17 days (range 5-66 days) for non-responders (p<0.01). Nevertheless, all patients died. Causes of death were progressive GVHD in 7 patients (47%), infection in 6 patients (40%), cardiac death in 1 patient (6.7%) and relapse in 1 patient (6,7%).
Second-line treatment with etanercept does induce responses in SR-aGVHD of the gut but appears to be associated with poor long-term survival even in responding patients.
急性移植物抗宿主病(aGVHD)是异基因干细胞移植(alloSCT)的一种重要并发症。目前推荐高剂量糖皮质激素作为II-IV级aGVHD的一线治疗,40%-50%的患者可实现总体完全缓解(CR)。尚未确立标准的二线治疗方案。已报道了不同的选择,包括抗TNFα抗体。
我们回顾性分析了在我院接受依那西普治疗的15例激素难治性(SR)aGVHD患者的结局。患者因血液系统恶性肿瘤接受移植,接受了清髓或非清髓预处理方案。移植物抗宿主病的预防包括环孢素A和霉酚酸。
急性移植物抗宿主病在移植后中位61天被诊断。所有患者均有肠道III级aGVHD。依那西普二线治疗在一线治疗开始后中位13天开始。总体缓解率为53%,3例患者完全缓解,5例患者部分缓解。整个组在开始依那西普治疗后的中位总生存期为66天(范围5-267天)。缓解者的中位总生存期为99天(范围47-267天),未缓解者为17天(范围5-66天)(p<0.01)。然而,所有患者均死亡。死亡原因包括7例患者(47%)的进行性移植物抗宿主病、6例患者(40%)的感染、1例患者(6.7%)的心源性死亡和1例患者(6.7%)的复发。
依那西普二线治疗确实可在肠道SR-aGVHD中诱导缓解,但即使是缓解患者,其长期生存率似乎也较低。