Federal University of Minas Gerais, School of Economics, Center of post-graduate and Research in Administration, Belo Horizonte, Minas Gerais, Brazil.
Business Administration Department - Observatory of human resources for health, Universidade Federal de Minas Gerais, Antonio Carlos, avenue, 6627, Belo Horizonte, Minas Gerais, Brazil.
BMC Cancer. 2017 Oct 30;17(1):706. doi: 10.1186/s12885-017-3700-z.
Oral cancer is a potentially fatal disease, especially when diagnosed in advanced stages. In Brazil, the primary health care (PHC) system is responsible for promoting oral health in order to prevent oral diseases. However, there is insufficient evidence to assess whether actions of the PHC system have some effect on the morbidity and mortality from oral cancer. The purpose of this study was to analyze the effect of PHC structure and work processes on the incidence and mortality rates of oral cancer after adjusting for contextual variables.
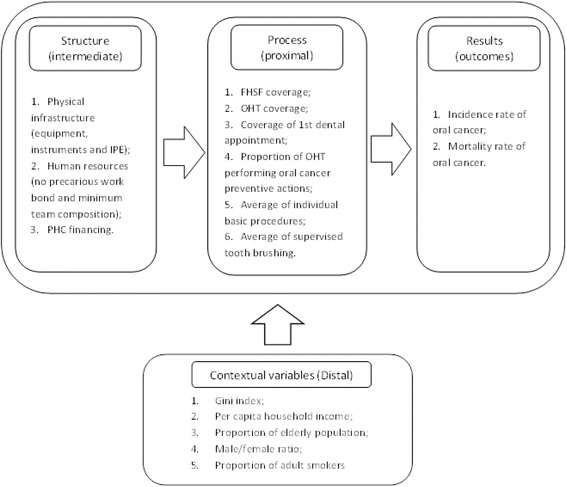
An ecological, longitudinal and analytical study was carried out. Data were obtained from different secondary data sources, including three surveys that were nationally representative of Brazilian PHC and carried out over the course of 10 years (2002-2012). Data were aggregated at the state level at different times. Oral cancer incidence and mortality rates, standardized by age and gender, served as the dependent variables. Covariables (sociodemographic, structure of basic health units, and work process in oral health) were entered in the regression models using a hierarchical approach based on a theoretical model. Analysis of mixed effects with random intercept model was also conducted (alpha = 5%).
The oral cancer incidence rate was positively association with the proportion of of adults over 60 years (β = 0.59; p = 0.010) and adult smokers (β = 0.29; p = 0.010). The oral cancer related mortality rate was positively associated with the proportion of of adults over 60 years (β = 0.24; p < 0.001) and the performance of preventative and diagnostic actions for oral cancer (β = 0.02; p = 0.002). Mortality was inversely associated with the coverage of primary care teams (β = -0.01; p < 0.006) and PHC financing (β = -0.52; p = 0.014).
In Brazil, the PHC structure and work processes have been shown to help reduce the mortality rate of oral cancer, but not the incidence rate of the disease. We recommend expanding investments in PHC in order to prevent oral cancer related deaths.
口腔癌是一种潜在的致命疾病,尤其是在晚期诊断时。在巴西,初级卫生保健(PHC)系统负责促进口腔健康,以预防口腔疾病。然而,目前尚无足够的证据来评估 PHC 系统的行动是否对口腔癌的发病率和死亡率产生了一定的影响。本研究旨在分析 PHC 结构和工作流程对调整背景变量后的口腔癌发病率和死亡率的影响。
进行了一项生态、纵向和分析性研究。数据来自不同的二级数据源,包括三次在全国范围内具有代表性的巴西 PHC 调查,调查时间跨度为 10 年(2002-2012 年)。数据在不同时间按州一级进行汇总。年龄和性别标准化的口腔癌发病率和死亡率作为因变量。回归模型中纳入了协变量(社会人口统计学、基本保健单位结构和口腔卫生工作流程),采用基于理论模型的分层方法。还进行了混合效应分析(随机截距模型)(α=5%)。
口腔癌发病率与 60 岁以上成年人的比例呈正相关(β=0.59;p=0.010)和成年吸烟者(β=0.29;p=0.010)。口腔癌相关死亡率与 60 岁以上成年人的比例呈正相关(β=0.24;p<0.001)和口腔癌预防和诊断措施的实施呈正相关(β=0.02;p=0.002)。死亡率与初级保健团队的覆盖范围呈负相关(β=-0.01;p<0.006)和 PHC 融资呈负相关(β=-0.52;p=0.014)。
在巴西,PHC 结构和工作流程已被证明有助于降低口腔癌的死亡率,但不能降低发病率。我们建议增加对 PHC 的投资,以预防与口腔癌相关的死亡。