Departments of Radiology, Affiliated Tumor Hospital of Guangxi Medical University, Nanning 530021, Guangxi Zhuang Autonomous Region, China.
Hepatobiliary Surgery, Affiliated Tumor Hospital of Guangxi Medical University, Nanning 530021, Guangxi Zhuang Autonomous Region, China.
World J Gastroenterol. 2017 Sep 21;23(35):6467-6473. doi: 10.3748/wjg.v23.i35.6467.
To develop and validate a risk estimation of tumor recurrence following curative resection of operable hepatocellular carcinoma (HCC).
Data for 128 patients with operable HCC (according to Barcelona Clinic Liver Cancer imaging criteria) who underwent preoperative computed tomography (CT) evaluation at our hospital from May 1, 2013 through May 30, 2014 were included in this study. Follow-up data were obtained from hospital medical records. Follow-up data through May 30, 2016 were used to retrospectively analyze preoperative multiphasic CT findings, surgical histopathology results, and serum α-fetoprotein and thymidine kinase-1 levels. The χ test, independent -test, and Mann-Whitney test were used to analyze data. A -value of < 0.05 was considered statistically significant.
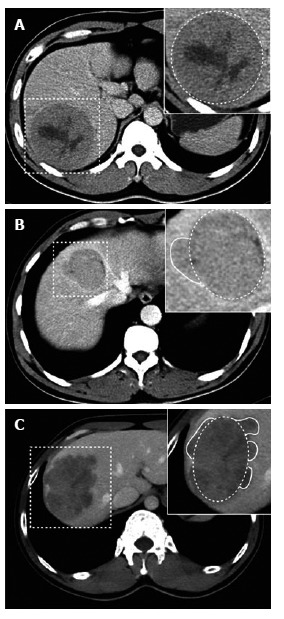
During the follow-up period, 38 of 128 patients (29.7%) had a postoperative HCC recurrence. Microvascular invasion (MVI) was associated with HCC recurrence (χ = 13.253, < 0.001). Despite postoperative antiviral therapy and chemotherapy, 22 of 44 patients with MVI experienced recurrence after surgical resection. The presence of MVI was 57.9% sensitive, 75.6% specific and 70.3% accurate in predicting postoperative recurrence. Of 84 tumors without MVI, univariate analysis confirmed that tumor margins, tumor margin grade, and tumor capsule detection on multiphasic CT were associated with HCC recurrence ( < 0.05). Univariate analyses showed no difference between groups with respect to hepatic capsular invasion, Ki-67 proliferation marker value, Edmondson-Steiner grade, largest tumor diameter, necrosis, arterial phase enhanced ratio, portovenous phase enhanced ratio, peritumoral enhancement, or serum α-fetoprotein level.
Non-smooth tumor margins, incomplete tumor capsules and missing tumor capsules correlated with postoperative HCC recurrence. HCC recurrence following curative resection may be predicted using CT.
开发并验证可切除肝细胞癌(HCC)术后肿瘤复发风险的评估方法。
纳入 2013 年 5 月 1 日至 2014 年 5 月 30 日在我院接受术前计算机断层扫描(CT)评估的 128 例可切除 HCC 患者的数据。通过医院病历获得随访数据。使用回顾性分析术前多期 CT 发现、手术组织病理学结果、血清甲胎蛋白和胸苷激酶-1 水平的方法对截至 2016 年 5 月 30 日的随访数据进行分析。采用卡方检验、独立样本 t 检验和曼-惠特尼 U 检验对数据进行分析。以 P<0.05 为差异有统计学意义。
在随访期间,128 例患者中有 38 例(29.7%)发生术后 HCC 复发。微血管侵犯(MVI)与 HCC 复发相关(χ=13.253,P<0.001)。尽管术后进行抗病毒治疗和化疗,44 例 MVI 患者中有 22 例在手术切除后复发。MVI 的存在对预测术后复发的敏感性为 57.9%,特异性为 75.6%,准确性为 70.3%。在 84 例无 MVI 的肿瘤中,单因素分析证实多期 CT 上肿瘤边缘、肿瘤边缘分级和肿瘤包膜检测与 HCC 复发相关(P<0.05)。单因素分析显示,两组在肝包膜侵犯、Ki-67 增殖标志物值、Edmondson-Steiner 分级、最大肿瘤直径、坏死、动脉期增强率、门静脉期增强率、肿瘤周围增强和血清甲胎蛋白水平方面无差异。
非光滑肿瘤边缘、不完整肿瘤包膜和缺失肿瘤包膜与术后 HCC 复发相关。CT 可用于预测根治性切除术后 HCC 的复发。