Institute of Gastroenterology and Hepatology, "St. Spiridon" Hospital, "Grigore T. Popa" University of Medicine and Pharmacy, 700111 Iasi, Romania.
Institute of Gastroenterology and Hepatology, "St. Spiridon" Hospital, 700111 Iasi, Romania.
World J Gastroenterol. 2017 Sep 21;23(35):6500-6515. doi: 10.3748/wjg.v23.i35.6500.
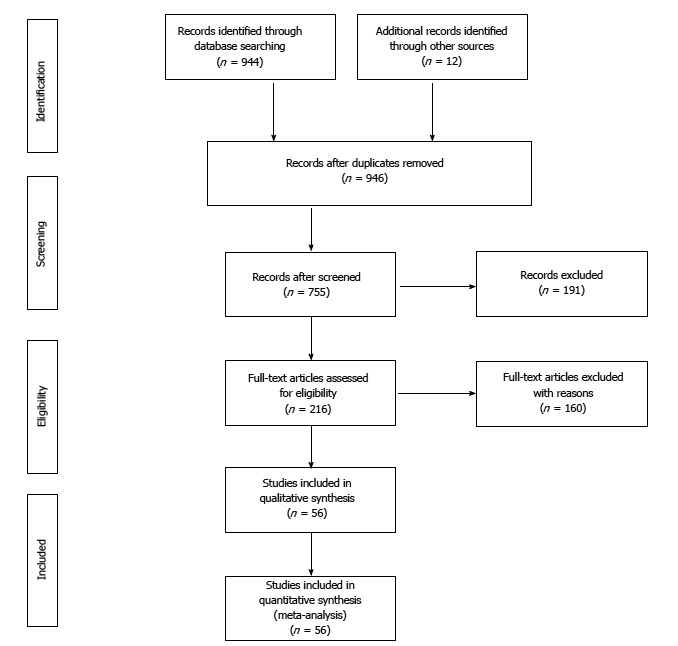
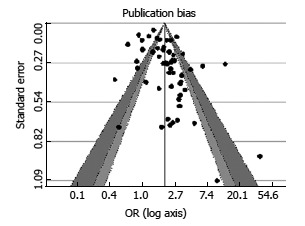
To perform a systematic review and meta-analysis on proton pump inhibitors (PPIs) therapy and the risk of infection (CDI). METHODS We conducted a systematic search of MEDLINE/PubMed and seven other databases through January 1990 to March 2017 for published studies that evaluated the association between PPIs and CDI. Adult case-control and cohort studies providing information on the association between PPI therapy and the development of CDI were included. Pooled odds ratios (ORs) estimates with 95% confidence intervals (CIs) were calculated using the random effect. Heterogeneity was assessed by test and Cochran's statistic. Potential publication bias was evaluated funnel plot, and quality of studies by the Newcastle-Otawa Quality Assessment Scale (NOS).
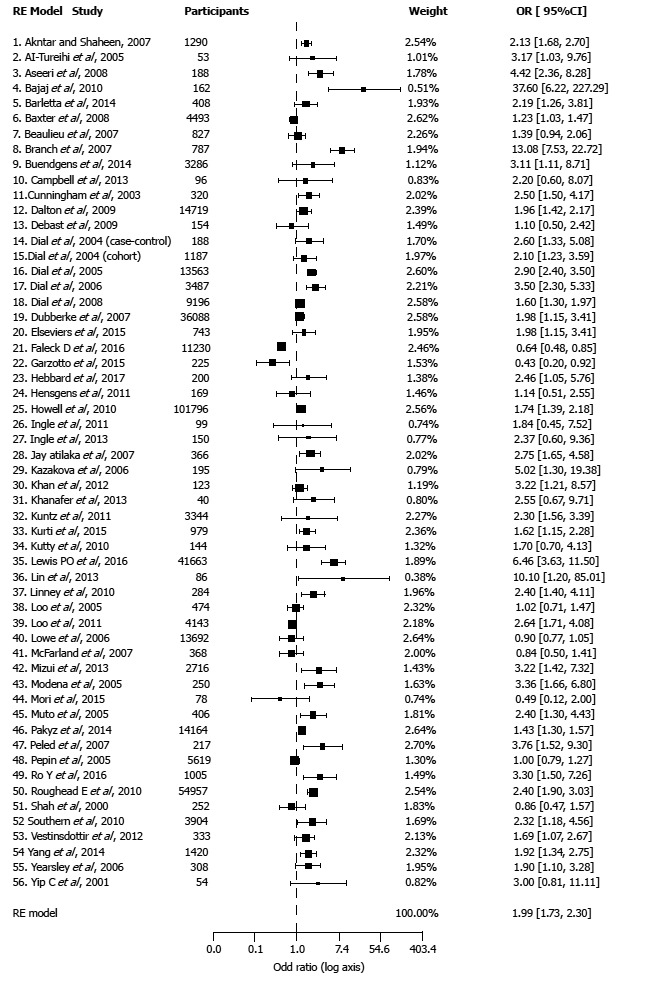
Fifty-six studies (40 case-control and 16 cohort) involving 356683 patients met the inclusion criteria and were analyzed. Both the overall pooled estimates and subgroup analyses showed increased risk for CDI despite substantial statistical heterogeneity among studies. Meta-analysis of all studies combined showed a significant association between PPI users and the risk of CDI (pooled OR = 1.99, CI: 1.73-2.30, < 0.001) as compared with non-users. The association remained significant in subgroup analyses: by design-case-control (OR = 2.00, CI: 1.68-2.38, < 0.0001), and cohort (OR = 1.98, CI: 1.51-2.59, < 0.0001); adjusted (OR = 1.95, CI: 1.67-2.27, < 0.0001) and unadjusted (OR = 2.02, CI: 1.41-2.91, 0.0001); unicenter (OR = 2.18, CI: 1.72-2.75, 0.0001) and multicenter (OR = 1.82, CI: 1.51-2.19, P < 0.0001); age ≥ 65 years (OR = 1.93, CI: 1.40-2.68, 0.0001) and < 65 years (OR = 2.06, CI: 1.11-3.81, 0.01). No significant differences were found in subgroup analyses (test for heterogeneity): 0.93 for case-control cohort, 0.85 for adjusted unadjusted, 0.24 for unicenter multicenter, 0.86 for age ≥ 65 years and < 65 years. There was significant heterogeneity across studies ( = 85.4%, 0.001) as well as evidence of publication bias (funnel plot asymmetry test, 0.002).
This meta-analysis provides further evidence that PPI use is associated with an increased risk for development of CDI. Further high-quality, prospective studies are needed to assess whether this association is causal.
对质子泵抑制剂(PPIs)治疗与感染(CDI)风险的关系进行系统评价和荟萃分析。方法:我们系统地检索了 MEDLINE/PubMed 和其他七个数据库,检索时间为 1990 年 1 月至 2017 年 3 月,以获取评估 PPI 治疗与 CDI 之间关联的已发表研究。纳入了提供 PPI 治疗与 CDI 发展之间关联信息的成人病例对照和队列研究。使用随机效应模型计算了合并的优势比(OR)估计值及其 95%置信区间(CI)。通过 检验和 Cochrane's 统计量评估异质性。通过漏斗图评估潜在的发表偏倚,并使用纽卡斯尔-渥太华质量评估量表(NOS)评估研究质量。
共有 56 项研究(40 项病例对照和 16 项队列研究)纳入了 356683 名患者,符合纳入标准并进行了分析。尽管研究之间存在显著的统计学异质性,但总体合并估计值和亚组分析均显示 CDI 的风险增加。所有研究的荟萃分析表明,与非使用者相比,PPI 使用者与 CDI 风险之间存在显著关联(合并 OR = 1.99,CI:1.73-2.30,<0.001)。在亚组分析中,这种关联仍然显著:设计为病例对照(OR = 2.00,CI:1.68-2.38,<0.0001)和队列(OR = 1.98,CI:1.51-2.59,<0.0001);调整(OR = 1.95,CI:1.67-2.27,<0.0001)和未调整(OR = 2.02,CI:1.41-2.91,<0.0001);单中心(OR = 2.18,CI:1.72-2.75,<0.0001)和多中心(OR = 1.82,CI:1.51-2.19,<0.0001);年龄≥65 岁(OR = 1.93,CI:1.40-2.68,<0.0001)和<65 岁(OR = 2.06,CI:1.11-3.81,0.01)。在亚组分析(异质性检验)中未发现显著差异:病例对照与队列( = 0.93)、调整与未调整( = 0.85)、单中心与多中心( = 0.24)、年龄≥65 岁与<65 岁( = 0.86)。研究之间存在显著的异质性( = 85.4%,<0.001),且存在发表偏倚的证据(漏斗图不对称检验,<0.002)。
本荟萃分析进一步提供了证据表明,PPI 治疗与 CDI 的发生风险增加有关。需要进一步开展高质量的前瞻性研究,以评估这种关联是否具有因果关系。