Yagyu Takeshi, Kumada Masahiro, Nakagawa Tsutomu
Department of Cardiology, Toyonaka Municipal Hospital, Toyonaka, Osaka, Japan.
PLoS One. 2017 Nov 2;12(11):e0187410. doi: 10.1371/journal.pone.0187410. eCollection 2017.
Patients with acute heart failure (AHF) show various clinical courses during hospitalization. We aimed to identify time course predictors of in-hospital mortality and to establish a sequentially assessable risk model.
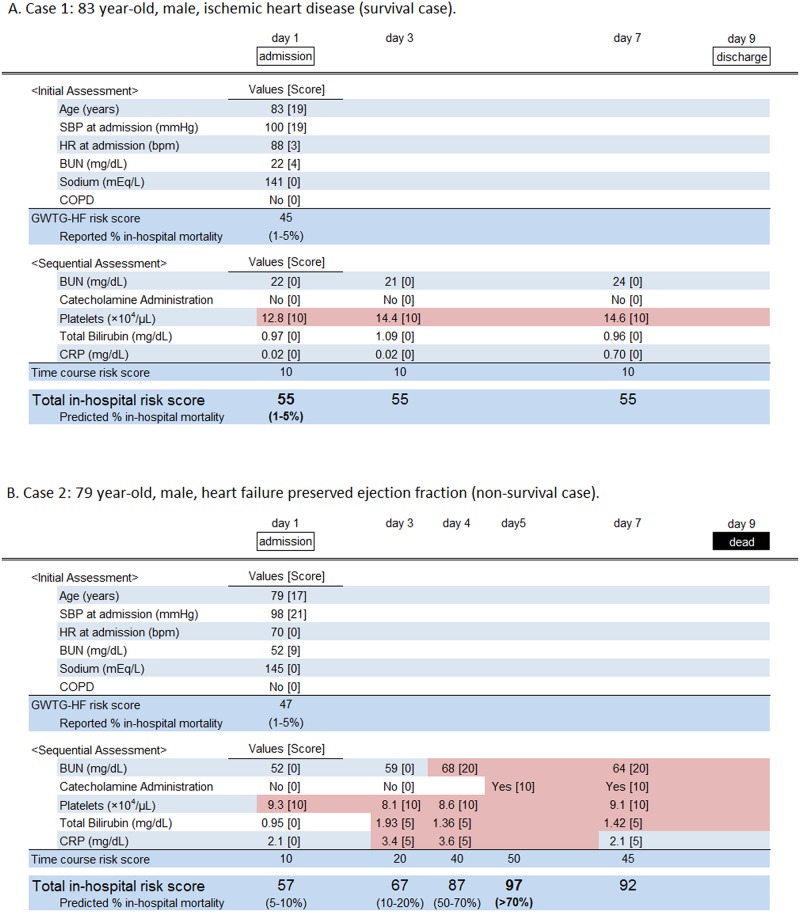
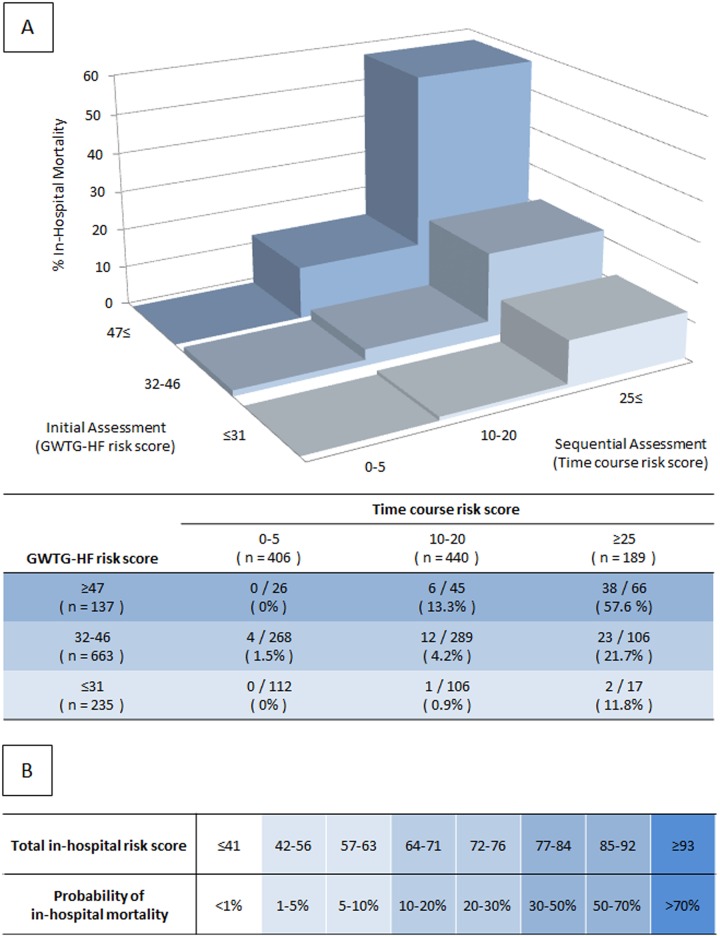
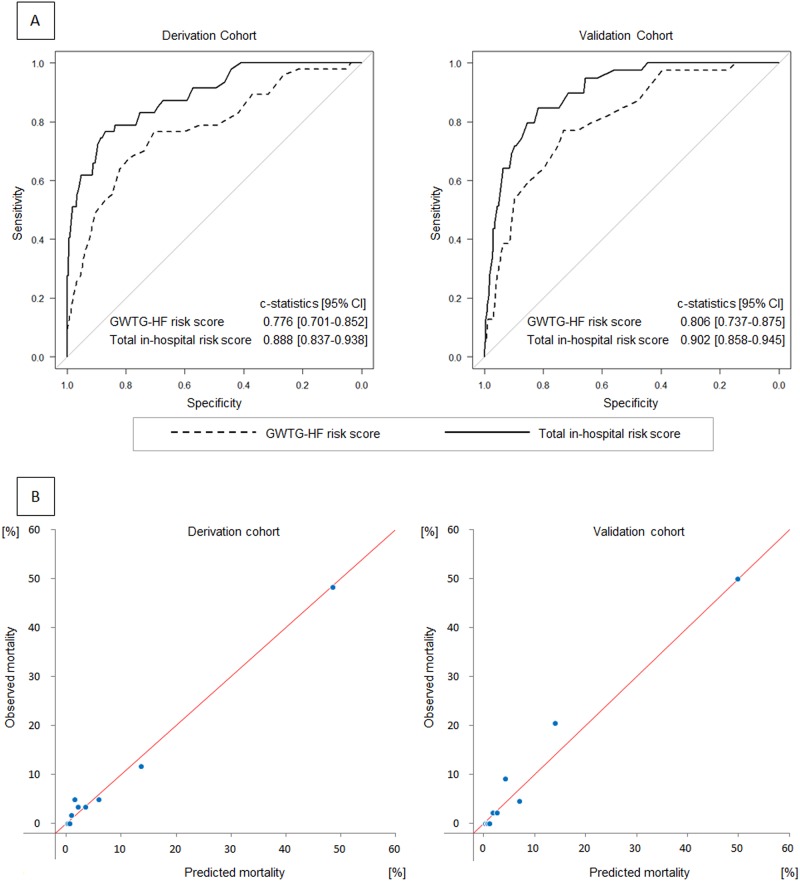
We enrolled 1,035 consecutive AHF patients into derivation (n = 597) and validation (n = 438) cohorts. For risk assessments at admission, we utilized Get With the Guidelines-Heart Failure (GWTG-HF) risk scores. We examined significant predictors of in-hospital mortality from 11 variables obtained during hospitalization and developed a risk stratification model using multiple logistic regression analysis. Across both cohorts, 86 patients (8.3%) died during hospitalization. Using backward stepwise selection, we identified five time-course predictors: catecholamine administration, minimum platelet concentration, maximum blood urea nitrogen, total bilirubin, and C-reactive protein levels; and established a time course risk score that could sequentially assess a patient's risk status. The addition of a time course risk score improved the discriminative ability of the GWTG-HF risk score (c-statistics in derivation and validation cohorts: 0.776 to 0.888 [p = 0.002] and 0.806 to 0.902 [p<0.001], respectively). A calibration plot revealed a good relationship between observed and predicted in-hospital mortalities in both cohorts (Hosmer-Lemeshow chi-square statistics: 6.049 [p = 0.642] and 5.993 [p = 0.648], respectively). In each group of initial low-intermediate risk (GWTG-HF risk score <47) and initial high risk (GWTG-HF risk score ≥47), in-hospital mortality was about 6- to 9-fold higher in the high time course risk score group than in the low-intermediate time course risk score group (initial low-intermediate risk group: 20.3% versus 2.2% [p<0.001], initial high risk group: 57.6% versus 8.5% [p<0.001]).
A time course assessment related to in-hospital mortality during the hospitalization of AHF patients can clearly categorize a patient's on-going status, and may assist patients and clinicians in deciding treatment options.
急性心力衰竭(AHF)患者在住院期间表现出不同的临床病程。我们旨在确定院内死亡的时间进程预测因素,并建立一个可顺序评估的风险模型。
我们将1035例连续的AHF患者纳入推导队列(n = 597)和验证队列(n = 438)。对于入院时的风险评估,我们使用了“遵循心力衰竭指南”(GWTG-HF)风险评分。我们检查了住院期间获得的11个变量中院内死亡的显著预测因素,并使用多元逻辑回归分析建立了一个风险分层模型。在两个队列中,共有86例患者(8.3%)在住院期间死亡。通过向后逐步选择,我们确定了五个时间进程预测因素:儿茶酚胺使用情况、最低血小板浓度、最高血尿素氮、总胆红素和C反应蛋白水平;并建立了一个可以顺序评估患者风险状态的时间进程风险评分。添加时间进程风险评分提高了GWTG-HF风险评分的辨别能力(推导队列和验证队列中的c统计量:分别从0.776提高到0.888 [p = 0.002]和从0.806提高到0.902 [p<0.001])。校准图显示两个队列中观察到的和预测的院内死亡率之间具有良好的关系(Hosmer-Lemeshow卡方统计量:分别为6.049 [p = 0.642]和5.993 [p = 0.648])。在初始低-中度风险组(GWTG-HF风险评分<47)和初始高风险组(GWTG-HF风险评分≥47)中,高时间进程风险评分组的院内死亡率比低-中度时间进程风险评分组高约6至9倍(初始低-中度风险组:20.3%对2.2% [p<0.001],初始高风险组:57.6%对8.5% [p<0.001])。
与AHF患者住院期间院内死亡相关的时间进程评估可以清楚地对患者的当前状态进行分类,并可能有助于患者和临床医生决定治疗方案。