Hotchen Andrew J, McNally Martin A, Sendi Parham
Bone Infection Unit, Nuffield Orthopaedic Centre, Oxford University Hospitals, Oxford, UK.
Addenbrooke's Hospital, Cambridge University Hospitals, Cambridge, UK.
J Bone Jt Infect. 2017 Sep 12;2(4):167-174. doi: 10.7150/jbji.21050. eCollection 2017.
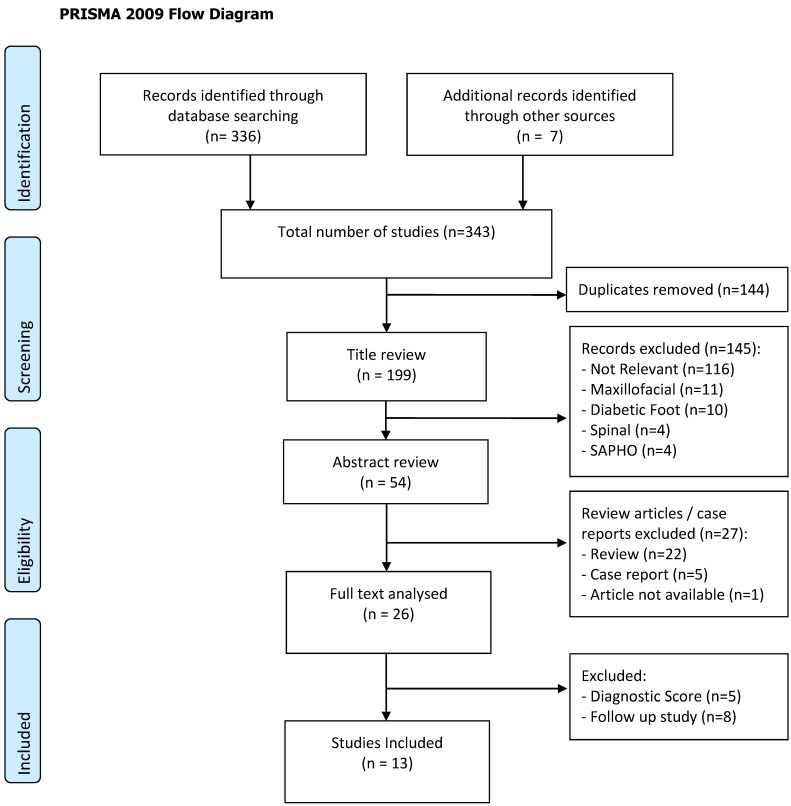
Osteomyelitis is a complex disease. Treatment involves a combination of bone resection, antimicrobials and soft-tissue coverage. There is a difficulty in unifying a classification system for long bone osteomyelitis that is generally accepted. In this systematic review, we aim to investigate the classification systems for long bone osteomyelitis that have been presented within the literature. By doing this, we hope to elucidate the important variables that are required when classifying osteomyelitis. A complete search of the Medline, EMBASE, Cochrane and Ovid databases was undertaken. Following exclusion criteria, 13 classification systems for long-bone osteomyelitis were included for review. The 13 classification systems that were included for review presented seven different variables that were used for classification. Ten of them used only one main variable, two used two variables and one used seven variables. The variables included bone involvement (used in 7 classification systems), acute versus chronic infection (used in 6), aetiopathogenesis (used in 3), host status (used in 3), soft tissue (used in 2), microbiology (used in 1) and location of infected bone (used in 1). The purpose of each classification system could be grouped as either descriptive (3 classification systems), prognostic (4) or for management (4). Two of the 13 classification systems were for both prognostic and management purposes. This systematic review has demonstrated a variety of variables used for classification of long bone osteomyelitis. While some variables are used to guide management and rehabilitation after surgery (e.g., bone defect, soft tissue coverage), others were postulated to provide prognostic information (e.g., host status). Finally, some variables were used for descriptive purposes only (aetiopathogenesis). In our view and from today's perspective, bone involvement, antimicrobial resistance patterns of causative micro-organisms, the need for soft-tissue coverage and host status are important variables to include in a classification system.
骨髓炎是一种复杂的疾病。治疗方法包括骨切除、使用抗菌药物以及软组织覆盖。目前难以统一一个被广泛接受的长骨骨髓炎分类系统。在本系统评价中,我们旨在研究文献中已提出的长骨骨髓炎分类系统。通过这样做,我们希望阐明骨髓炎分类时所需的重要变量。我们对Medline、EMBASE、Cochrane和Ovid数据库进行了全面检索。根据排除标准,纳入了13个长骨骨髓炎分类系统进行综述。纳入综述的13个分类系统呈现了7个用于分类的不同变量。其中10个仅使用一个主要变量,2个使用两个变量,1个使用7个变量。这些变量包括骨受累情况(7个分类系统使用)、急性与慢性感染(6个)、病因发病机制(3个)、宿主状态(3个)、软组织(2个)、微生物学(1个)以及感染骨的位置(1个)。每个分类系统的目的可归为描述性(3个分类系统)、预后性(4个)或用于管理(4个)。13个分类系统中有2个兼具预后和管理目的。本系统评价展示了用于长骨骨髓炎分类的多种变量。虽然一些变量用于指导术后管理和康复(如骨缺损、软组织覆盖),但其他一些变量则是为了提供预后信息(如宿主状态)。最后,一些变量仅用于描述目的(病因发病机制)。从我们的观点以及当今的角度来看,骨受累情况、致病微生物的抗菌耐药模式、软组织覆盖的需求以及宿主状态是分类系统中应纳入的重要变量。