Zhao Bo, Maquilan Genevieve, Jiang Steve, Schwartz David L
Department of Radiation Oncology, The University of Texas Southwestern Medical Center, Dallas, TX, USA.
Department of Radiation Oncology, University of Tennessee Health Science Center-West Cancer Center, Memphis, TN, USA.
J Appl Clin Med Phys. 2018 Jan;19(1):17-24. doi: 10.1002/acm2.12211. Epub 2017 Nov 9.
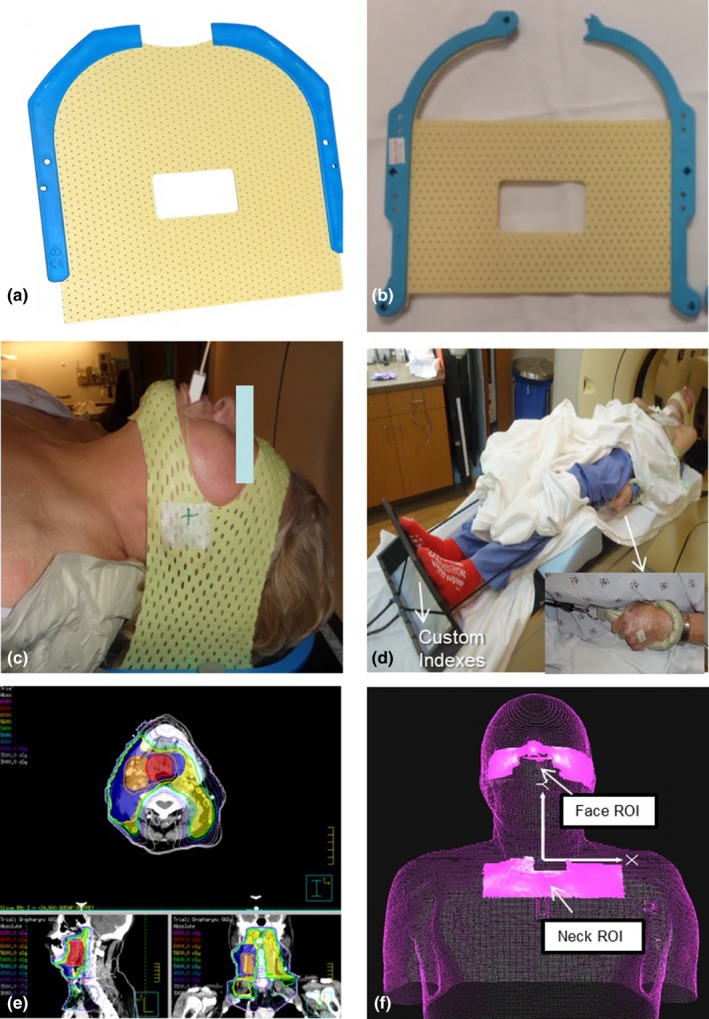
Full face and neck thermoplastic masks provide standard-of-care immobilization for patients receiving H&N IMRT. However, these masks are uncomfortable and increase skin dose. The purpose of this pilot trial was to investigate the feasibility and setup accuracy of minimal face and neck mask immobilization with optical surface guidance.
Twenty patients enrolled onto this IRB-approved protocol. Patients were immobilized with masks securing only forehead and chin. Shoulder movement was restricted by either moldable cushion or hand held strap retractors. Positional information, including isocenter location and CT skin contours, were imported to a commercial surface image guidance system. Patients typically received standard-of-care IMRT to 60-70 Gy in 30-33 fractions. Patients were first set up to surface markings with optical image guidance referenced to regions of interest (ROIs) on simulation CT images. Positioning was confirmed by in-room CBCT. Following six-dimensional robotic couch correction, a new optical real-time surface image was acquired to track intrafraction motion and to serve as a reference surface for setup at the next treatment fraction. Therapists manually recorded total treatment time as well as couch shifts based on kV imaging. Intrafractional ROI motion tracking was automatically recorded by the optical image guidance system. Patient comfort was assessed by self-administered surveys.
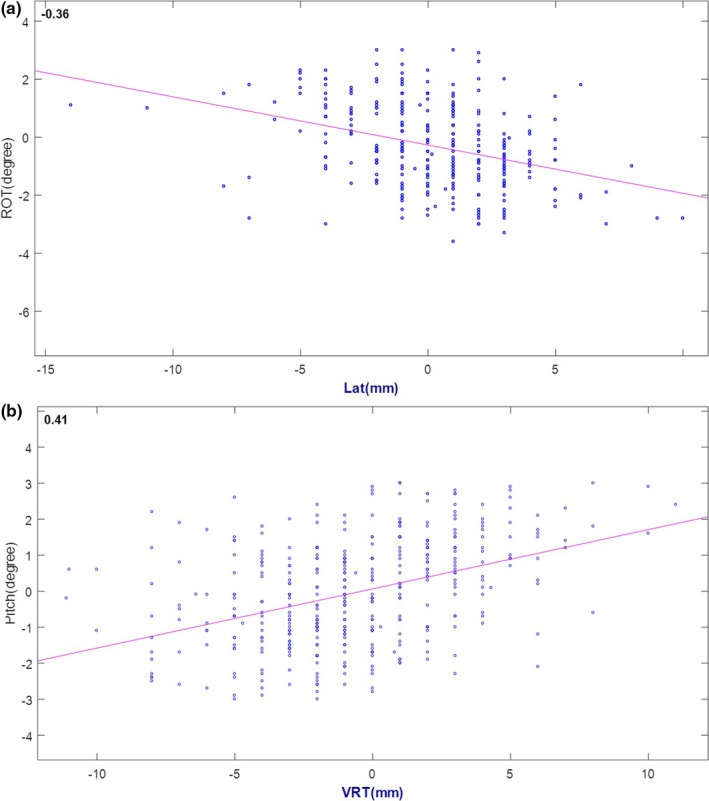
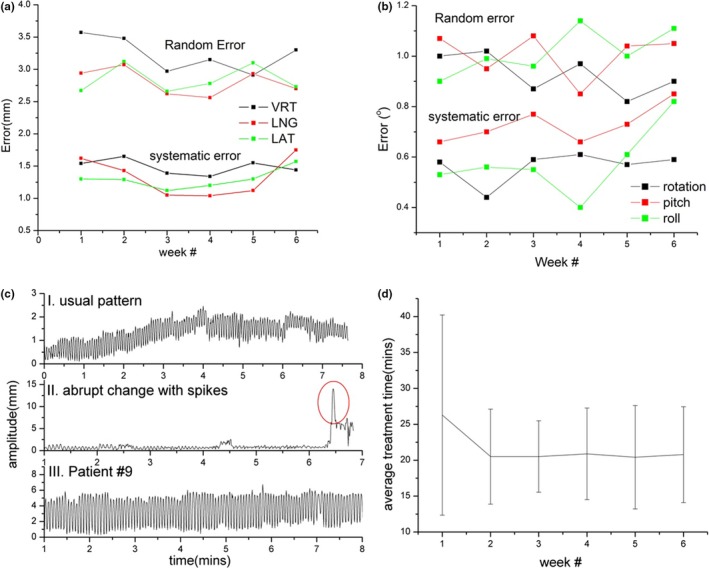
Setup error was measured as six-dimensional shifts (vertical/longitudinal/lateral/rotation/pitch/roll). Mean error values were -0.51 ± 2.42 mm, -0.49 ± 3.30 mm, 0.23 ± 2.58 mm, -0.15 ± 1.01 , -0.02 ± 1.19 , and 0.06 ± 1.08 , respectively. Average treatment time was 21.6 ± 8.4 mins). Subjective comfort during surface-guided treatment was confirmed on patient surveys.
These pilot results confirm feasibility of minimal mask immobilization combined with commercially available optical image guidance. Patient acceptance of minimal mask immobilization has been encouraging. Follow-up validation, with direct comparison to standard mask immobilization, appears warranted.
全脸和颈部热塑性面罩为接受头颈部调强放疗(H&N IMRT)的患者提供了标准的固定方式。然而,这些面罩佩戴起来不舒服,还会增加皮肤剂量。这项初步试验的目的是研究使用光学表面引导技术进行最小化面部和颈部面罩固定的可行性和摆位精度。
20名患者纳入了这项经机构审查委员会(IRB)批准的方案。患者使用仅固定额头和下巴的面罩进行固定。通过可塑形垫子或手持式束带牵开器限制肩部运动。包括等中心位置和CT皮肤轮廓在内的位置信息被导入到一个商用表面图像引导系统中。患者通常接受标准的调强放疗,剂量为60 - 70 Gy,分30 - 33次照射。患者首先通过光学图像引导,参照模拟CT图像上的感兴趣区域(ROI),摆位到体表标记处。通过室内锥形束CT(CBCT)确认定位。在进行六维机器人治疗床校正后,获取新的光学实时表面图像,以跟踪分次治疗期间的运动,并作为下一次治疗分次摆位的参考表面。治疗师根据千伏成像手动记录总治疗时间以及治疗床的移动。光学图像引导系统自动记录分次治疗期间感兴趣区域的运动跟踪情况。通过患者自行填写的调查问卷评估患者的舒适度。
摆位误差以六维位移(垂直/纵向/横向/旋转/俯仰/滚动)来衡量。平均误差值分别为-0.51±2.42毫米、-0.49±3.30毫米、0.23±2.58毫米、-0.15±1.01、-0.02±1.19和0.06±1.08。平均治疗时间为21.6±8.4分钟。患者调查问卷证实了表面引导治疗期间的主观舒适度。
这些初步结果证实了最小化面罩固定结合商用光学图像引导技术的可行性。患者对最小化面罩固定的接受度令人鼓舞。与标准面罩固定进行直接比较的后续验证似乎是有必要的。