Centre for Primary Care and Public Health, Queen Mary University of London, London, UK.
Department of Medical Statistics, London School of Hygiene and Tropical Medicine, London, UK.
BMJ Open. 2017 Nov 8;7(11):e016970. doi: 10.1136/bmjopen-2017-016970.
To systematically review the quality of reporting of pilot and feasibility of cluster randomised trials (CRTs). In particular, to assess (1) the number of pilot CRTs conducted between 1 January 2011 and 31 December 2014, (2) whether objectives and methods are appropriate and (3) reporting quality.
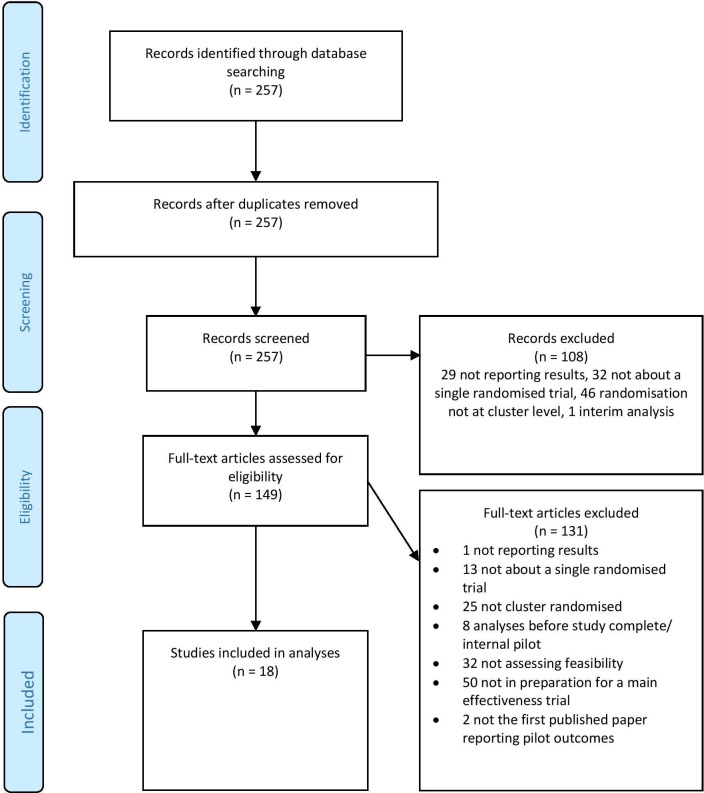
We searched PubMed (2011-2014) for CRTs with 'pilot' or 'feasibility' in the title or abstract; that were assessing some element of feasibility and showing evidence the study was in preparation for a main effectiveness/efficacy trial. Quality assessment criteria were based on the Consolidated Standards of Reporting Trials (CONSORT) extensions for pilot trials and CRTs.
Eighteen pilot CRTs were identified. Forty-four per cent did not have feasibility as their primary objective, and many (50%) performed formal hypothesis testing for effectiveness/efficacy despite being underpowered. Most (83%) included 'pilot' or 'feasibility' in the title, and discussed implications for progression from the pilot to the future definitive trial (89%), but fewer reported reasons for the randomised pilot trial (39%), sample size rationale (44%) or progression criteria (17%). Most defined the cluster (100%), and number of clusters randomised (94%), but few reported how the cluster design affected sample size (17%), whether consent was sought from clusters (11%), or who enrolled clusters (17%).
That only 18 pilot CRTs were identified necessitates increased awareness of the importance of conducting and publishing pilot CRTs and improved reporting. Pilot CRTs should primarily be assessing feasibility, avoiding formal hypothesis testing for effectiveness/efficacy and reporting reasons for the pilot, sample size rationale and progression criteria, as well as enrolment of clusters, and how the cluster design affects design aspects. We recommend adherence to the CONSORT extensions for pilot trials and CRTs.
系统评价试点和可行性簇随机试验(CRT)的报告质量。特别是,评估(1)2011 年 1 月 1 日至 2014 年 12 月 31 日期间进行的试点 CRT 的数量,(2)目标和方法是否合适,以及(3)报告质量。
我们在 PubMed 中搜索了标题或摘要中带有“试点”或“可行性”的 CRT;评估了可行性的某些要素,并表明该研究正在为主要的有效性/功效试验做准备。质量评估标准基于 CONSORT 对试点试验和 CRT 的扩展。
确定了 18 项试点 CRT。44%的研究没有将可行性作为主要目标,尽管研究力量不足,但许多研究(50%)对有效性/功效进行了正式的假设检验。大多数(83%)在标题中包含“试点”或“可行性”,并讨论了从试点到未来确定性试验的进展的影响(89%),但较少报告了随机试点试验的原因(39%),样本量理由(44%)或进展标准(17%)。大多数研究都定义了集群(100%)和随机化的集群数量(94%),但很少有研究报告集群设计如何影响样本量(17%),是否向集群征求了同意(11%),或者谁招募了集群(17%)。
仅确定了 18 项试点 CRT,这就需要提高对开展和发表试点 CRT 的重要性的认识,并提高报告质量。试点 CRT 应主要评估可行性,避免对有效性/功效进行正式的假设检验,并报告试点的原因、样本量理由和进展标准,以及集群的招募情况,以及集群设计如何影响设计方面。我们建议遵守 CONSORT 对试点试验和 CRT 的扩展。