National Institute for Health Research Liver Biomedical Research Unit, University Hospitals Birmingham NHS Foundation Trust and the University of Birmingham, Birmingham, UK; Centre for Liver Research, Institute of Immunology and Immunotherapy, University of Birmingham, Birmingham, UK; Liver Unit, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK.
National Institute for Health Research Liver Biomedical Research Unit, University Hospitals Birmingham NHS Foundation Trust and the University of Birmingham, Birmingham, UK; University of Birmingham, NIHR Liver BRU Clinical trials group, Cancer Research UK Clinical Trials Unit, Birmingham, UK.
Lancet Gastroenterol Hepatol. 2018 Jan;3(1):25-36. doi: 10.1016/S2468-1253(17)30326-6. Epub 2017 Nov 7.
Results of small-scale studies have suggested that stem-cell therapy is safe and effective in patients with liver cirrhosis, but no adequately powered randomised controlled trials have been done. We assessed the safety and efficacy of granulocyte colony-stimulating factor (G-CSF) and haemopoietic stem-cell infusions in patients with liver cirrhosis.
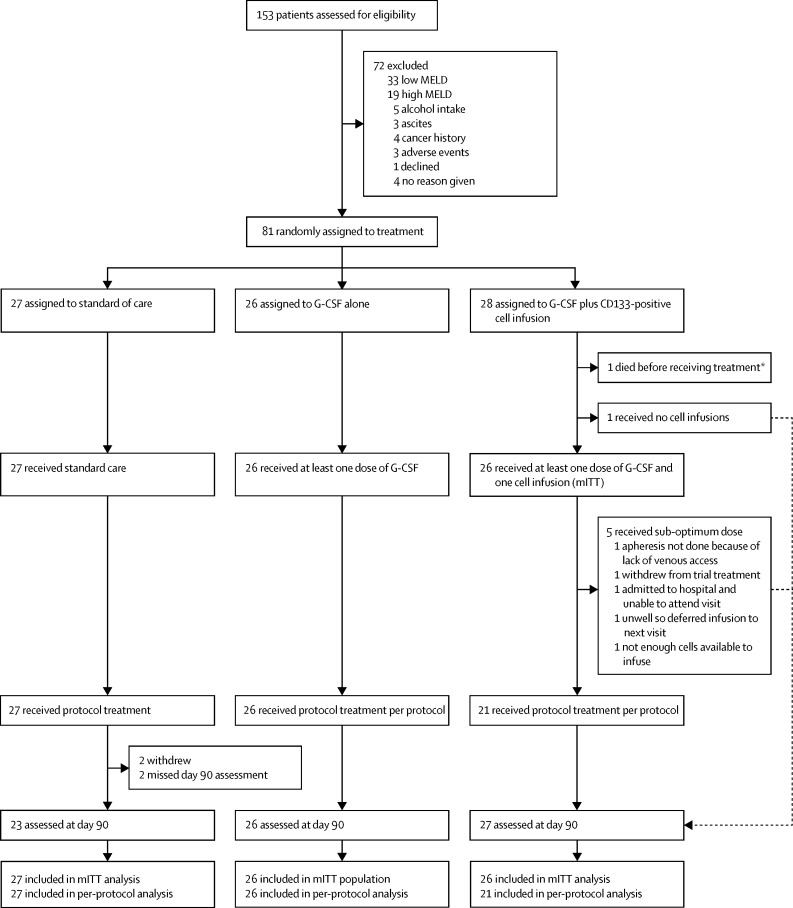
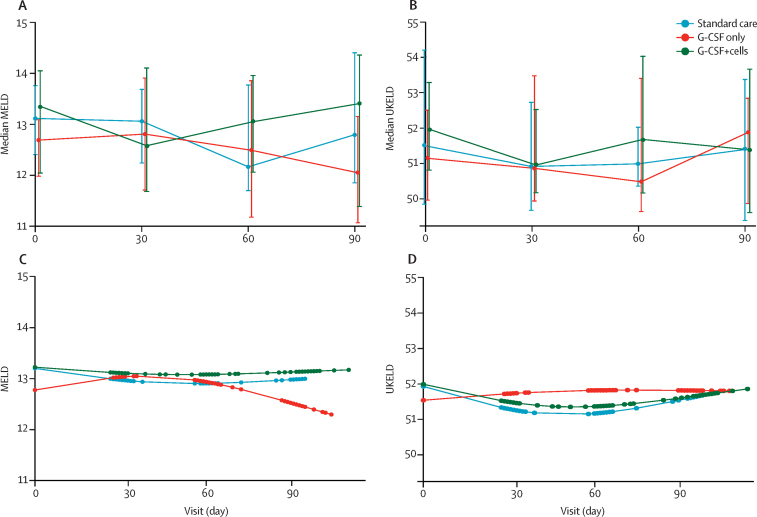
This multicentre, open-label, randomised, controlled phase 2 trial was done in three UK hospitals and recruited patients with compensated liver cirrhosis and MELD scores of 11·0-15·5. Patients were randomly assigned (1:1:1) to receive standard care (control), treatment with subcutaneous G-CSF (lenograstim) 15 μg/kg for 5 days, or treatment with G-CSF for 5 days followed by leukapheresis and intravenous infusion of three doses of CD133-positive haemopoietic stem cells (0·2 × 10 cells per kg per infusion). Randomisation was done by Cancer Research UK Clinical Trials Unit staff with a minimisation algorithm that stratified by trial site and cause of liver disease. The coprimary outcomes were improvement in severity of liver disease (change in MELD) at 3 months and the trend of change in MELD score over time. Analyses were done in the modified intention-to-treat population, which included all patients who received at least one day of treatment. Safety was assessed on the basis of the treatment received. This trial was registered at Current Controlled Trials on Nov 18, 2009; ISRCTN, number 91288089; and the European Clinical Trials Database, number 2009-010335-41.
Between May 18, 2010, and Feb 26, 2015, 27 patients were randomly assigned to the standard care, 26 to the G-CSF group, and 28 to the G-CSF plus stem-cell infusion group. Median change in MELD from day 0 to 90 was -0·5 (IQR -1·5 to 1·1) in the standard care group, -0·5 (-1·7 to 0·5) in the G-CSF group, and -0·5 (-1·3 to 1·0) in the G-CSF plus stem-cell infusion group. We found no evidence of differences between the treatment groups and control group in the trends of MELD change over time (p=0·55 for the G-CSF group vs standard care and p=0·75 for the G-CSF plus stem-cell infusion group vs standard care). Serious adverse events were more frequent the in G-CSF and stem-cell infusion group (12 [43%] patients) than in the G-CSF (three [11%] patients) and standard care (three [12%] patients) groups. The most common serious adverse events were ascites (two patients in the G-CSF group and two patients in the G-CSF plus stem-cell infusion group, one of whom was admitted to hospital with ascites twice), sepsis (four patients in the G-CSF plus stem-cell infusion group), and encephalopathy (three patients in the G-CSF plus stem-cell infusion group, one of whom was admitted to hospital with encephalopathy twice). Three patients died, including one in the standard care group (variceal bleed) and two in the G-CSF and stem-cell infusion group (one myocardial infarction and one progressive liver disease).
G-CSF with or without haemopoietic stem-cell infusion did not improve liver dysfunction or fibrosis and might be associated with increased frequency of adverse events compared with standard care.
National Institute of Health Research, The Sir Jules Thorn Charitable Trust.
小规模研究结果表明,干细胞疗法在肝硬化患者中是安全且有效的,但目前仍缺乏充分有力的随机对照试验。我们评估了粒细胞集落刺激因子(G-CSF)和造血干细胞输注在肝硬化患者中的安全性和疗效。
这项多中心、开放性、随机、对照的 2 期临床试验在英国的 3 家医院进行,招募了 MELD 评分在 11.0-15.5 分之间、代偿性肝硬化的患者。患者以 1:1:1 的比例随机分配(1:1:1)接受标准治疗(对照组)、皮下注射 G-CSF(rhG-CSF,15μg/kg,连续 5 天)或 G-CSF 治疗 5 天后进行白细胞分离和静脉输注 3 剂 CD133 阳性造血干细胞(每次输注 0.2×10^6 个细胞/公斤)。随机分组由英国癌症研究中心临床试验单位的工作人员根据最小化算法进行,该算法按试验地点和肝病病因进行分层。主要疗效终点是 3 个月时肝脏疾病严重程度的改善(MELD 变化)和 MELD 评分随时间的变化趋势。分析在改良意向治疗人群中进行,该人群包括接受至少一天治疗的所有患者。安全性基于所接受的治疗进行评估。这项试验于 2009 年 11 月 18 日在 Current Controlled Trials 上注册,注册号为 ISRCTN,编号为 91288089;以及欧洲临床试验数据库,编号为 2009-010335-41。
2010 年 5 月 18 日至 2015 年 2 月 26 日,共有 27 例患者被随机分配至标准治疗组,26 例患者被随机分配至 G-CSF 组,28 例患者被随机分配至 G-CSF 联合造血干细胞输注组。标准治疗组从第 0 天到第 90 天的 MELD 中位数变化为-0.5(IQR-1.5 至 1.1),G-CSF 组为-0.5(-1.7 至 0.5),G-CSF 联合造血干细胞输注组为-0.5(-1.3 至 1.0)。我们发现治疗组与对照组之间在 MELD 变化的趋势上没有差异(G-CSF 组与标准治疗相比,p=0.55;G-CSF 联合造血干细胞输注组与标准治疗相比,p=0.75)。严重不良事件在 G-CSF 和造血干细胞输注组(12 例[43%]患者)比 G-CSF 组(3 例[11%]患者)和标准治疗组(3 例[12%]患者)更为常见。最常见的严重不良事件是腹水(G-CSF 组和 G-CSF 联合造血干细胞输注组各 2 例患者,其中 1 例腹水两次住院)、败血症(G-CSF 联合造血干细胞输注组 4 例患者)和肝性脑病(G-CSF 联合造血干细胞输注组 3 例患者,其中 1 例肝性脑病两次住院)。3 例患者死亡,其中 1 例在标准治疗组(静脉曲张出血),2 例在 G-CSF 和造血干细胞输注组(1 例心肌梗死和 1 例进行性肝病)。
与标准治疗相比,G-CSF 联合或不联合造血干细胞输注并未改善肝功能或纤维化,并且可能与不良事件的发生率增加相关。
英国国家卫生研究院,朱利叶斯·桑纳姆慈善信托基金。