Guest Julian F, Esteban Jaime, Manganelli Anton G, Novelli Andrea, Rizzardini Giuliano, Serra Miquel
Faculty of Life Sciences and Medicine, King's College, London, United Kingdom.
Catalyst Health Economics Consultants, Rickmansworth, Hertfordshire, United Kingdom.
PLoS One. 2017 Nov 14;12(11):e0187792. doi: 10.1371/journal.pone.0187792. eCollection 2017.
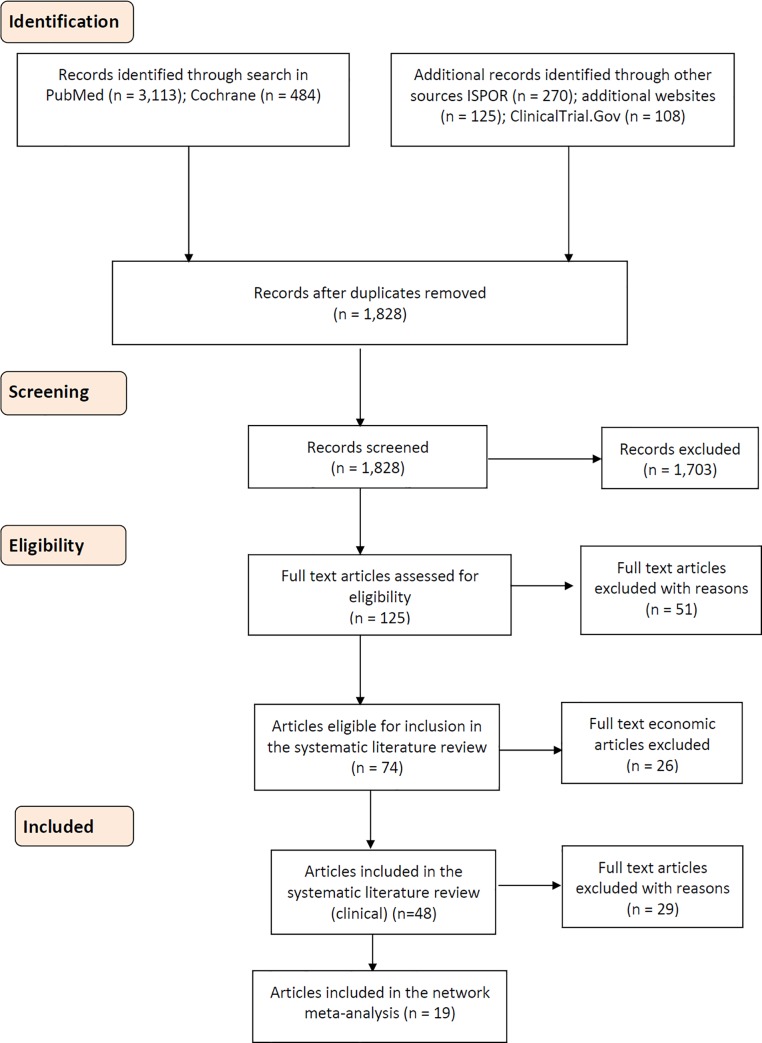
This NMA compared the efficacy and safety between IV antibiotics that are used in the current standard of care for managing adult patients (≥18 years of age) with ABSSSI.
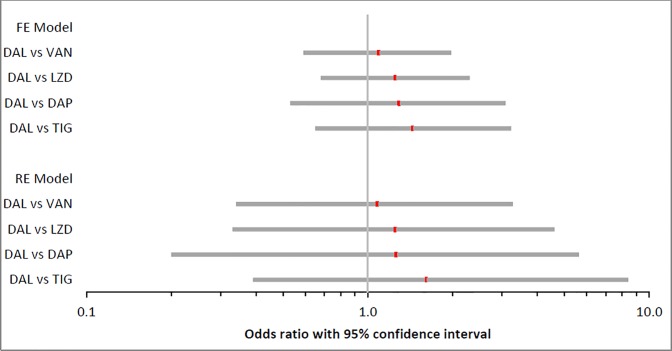
Comparators were chosen on the basis that both direct and indirect comparisons between the interventions of interest could be performed. Outcomes of the analysis were selected on the basis that they are frequently measured and reported in trials involving ABSSSI patients, and only published randomised control trials of any size and duration and with any blinding status were eligible for inclusion in the analysis. The NMA was performed using both a fixed-effect and random-effect model. Efficacy-related endpoints were (1) clinical treatment success and (2) microbiological success at TOC visit. Safety-related endpoints were (1) number of discontinuations due to AEs/SAEs, (2) patients experiencing AEs, (3) patients experiencing SAEs and (4) all-cause mortality.
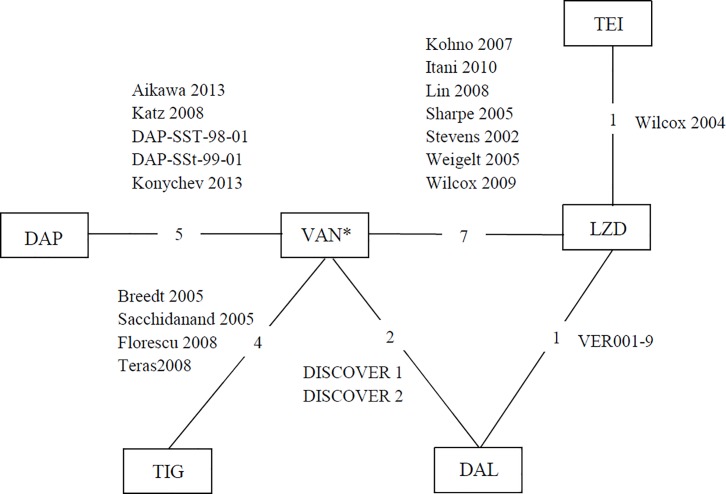
Study interventions included daptomycin, dalbavancin, linezolid and tigecycline. Vancomycin was the comparator in all studies, except in two where it was linezolid and teicoplanin. The NMA showed that irrespective of patient subgroup, the likelihood of clinical and microbiological success with dalbavancin was statistically similar to the comparators studied. No statistically significant differences were observed between dalbavancin and any of the comparators in the discontinuation rate due to AEs/SAEs. In contrast, dalbavancin was associated with a significantly lower likelihood of experiencing an AE than linezolid, a significantly lower likelihood of experiencing a SAE than vancomycin and daptomycin, and a significantly lower risk of all-cause mortality than vancomycin, linezolid and tigecycline.
Dalbavancin affords a promising, new alternative IV antimicrobial agent which is as effective as traditional therapies, but with the added benefit of enabling clinicians to treat patients with ABSSSI in different organisational settings. Notwithstanding, any introduction of an effective treatment with a differential mode of administration into healthcare systems must be followed by a change in clinical practice and patient management in order to fully achieve desirable economic outcomes.
本网络荟萃分析(NMA)比较了用于治疗成人(≥18岁)急性细菌性皮肤和皮肤结构感染(ABSSSI)现行标准治疗方案中的静脉用抗生素之间的疗效和安全性。
选择比较对象的依据是能够对感兴趣的干预措施进行直接和间接比较。分析结果的选择依据是它们在涉及ABSSSI患者的试验中经常被测量和报告,并且只有任何规模、持续时间和盲法状态的已发表随机对照试验才有资格纳入分析。使用固定效应模型和随机效应模型进行NMA。与疗效相关的终点为:(1)临床治疗成功;(2)在治疗结束时访视时的微生物学成功。与安全性相关的终点为:(1)因不良事件/严重不良事件而停药的数量;(2)发生不良事件的患者;(3)发生严重不良事件的患者;(4)全因死亡率。
研究干预措施包括达托霉素、达巴万星、利奈唑胺和替加环素。在所有研究中,万古霉素均为对照药物,但在两项研究中,对照药物为利奈唑胺和替考拉宁。NMA显示,无论患者亚组如何,达巴万星临床和微生物学成功的可能性在统计学上与所研究的对照药物相似。在因不良事件/严重不良事件导致的停药率方面,达巴万星与任何对照药物之间均未观察到统计学上的显著差异。相比之下,达巴万星发生不良事件的可能性显著低于利奈唑胺,发生严重不良事件的可能性显著低于万古霉素和达托霉素,全因死亡率风险显著低于万古霉素、利奈唑胺和替加环素。
达巴万星是一种有前景的新型静脉用抗菌药物,其疗效与传统疗法相当,但额外的好处是使临床医生能够在不同的组织环境中治疗ABSSSI患者。尽管如此,将任何具有不同给药方式的有效治疗方法引入医疗保健系统后,都必须随之改变临床实践和患者管理,以便充分实现理想的经济结果。