Infectious Disease Epidemiology Group, Weill Cornell Medicine-Qatar, Cornell University, Doha, Qatar.
London, United Kingdom.
Clin Infect Dis. 2018 Apr 3;66(8):1184-1191. doi: 10.1093/cid/cix975.
This study assessed levels, trends, and associations of observed syphilis prevalence in the general adult population using global pooled analyses.
A standardized database of syphilis prevalence was compiled by pooling systematically gathered data. Random-effects meta-analyses and meta-regressions were conducted using data from the period 1990-2016 to estimate pooled measures and assess predictors and trends. Countries were classified by World Health Organization region. Sensitivity analyses were conducted.
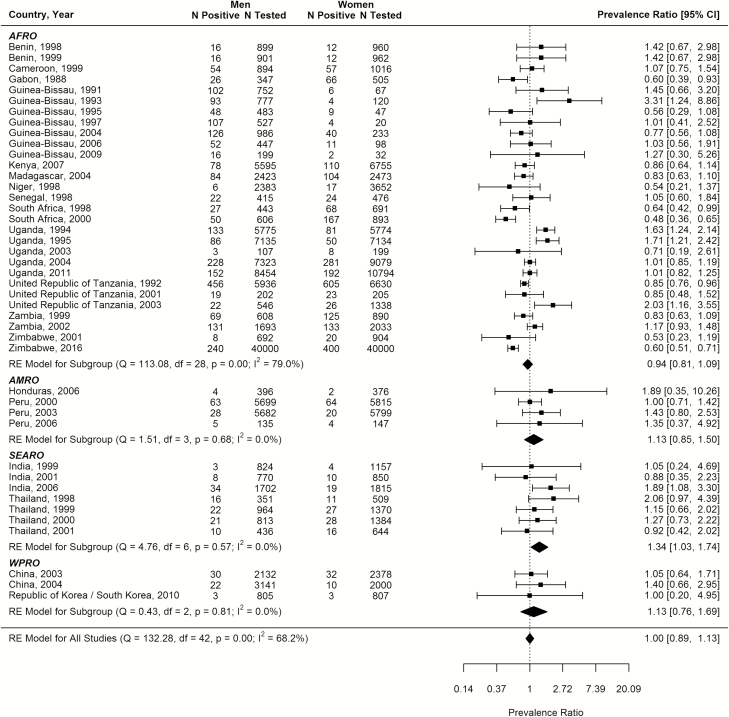
The database included 1103 prevalence measures from 136 million syphilis tests across 154 countries (85% from women in antenatal care). Global pooled mean prevalence (weighted by region population size) was 1.11% (95% confidence interval [CI], .99-1.22). Prevalence predictors were region, diagnostic assay, sample size, and calendar year interacting with region. Compared to the African Region, the adjusted odds ratio (AOR) was 0.42 (95% CI, .33-.54) for the Region of the Americas, 0.13 (95% CI, .09-.19) for the Eastern Mediterranean Region, 0.05 (95% CI, .03-.07) for the European Region, 0.21 (95% CI, .16-.28) for the South-East Asia Region, and 0.41 (95% CI, .32-.53) for the Western Pacific Region. Treponema pallidum hemagglutination assay (TPHA) only or rapid plasma reagin (RPR) only, compared with dual RPR/TPHA diagnosis, produced higher prevalence (AOR >1.26), as did smaller sample-size studies (<500 persons) (AOR >2.16). Prevalence declined in all regions; the annual AORs ranged from 0.84 (95% CI, .79-.90) in the Eastern Mediterranean to 0.97 (95% CI, .97-1.01) in the Western Pacific. The pooled mean male-to-female prevalence ratio was 1.00 (95% CI, .89-1.13). Sensitivity analyses confirmed robustness of results.
Syphilis prevalence has declined globally over the past 3 decades. Large differences in prevalence persist among regions, with the African Region consistently the most affected.
本研究使用全球汇总分析评估了一般成年人群中观察到的梅毒流行率的水平、趋势和相关性。
通过系统收集数据,编制了标准化的梅毒流行率数据库。使用 1990 年至 2016 年期间的数据进行随机效应荟萃分析和荟萃回归,以估计汇总指标并评估预测因素和趋势。根据世界卫生组织区域对国家进行分类。进行了敏感性分析。
该数据库包含来自 154 个国家的 13600 万次梅毒检测中的 1103 个流行率指标(85%来自产前护理中的女性)。全球汇总平均流行率(按区域人口规模加权)为 1.11%(95%置信区间[CI],0.99-1.22)。流行率预测因素为区域、诊断检测、样本量和与区域相互作用的日历年份。与非洲区域相比,调整后的优势比(AOR)分别为美洲区域 0.42(95%CI,0.33-0.54)、东地中海区域 0.13(95%CI,0.09-0.19)、欧洲区域 0.05(95%CI,0.03-0.07)、东南亚区域 0.21(95%CI,0.16-0.28)和西太平洋区域 0.41(95%CI,0.32-0.53)。与双重 RPR/TPHA 诊断相比,仅使用梅毒螺旋体血凝试验(TPHA)或快速血浆反应素(RPR)检测会导致更高的流行率(AOR>1.26),样本量较小的研究(<500 人)(AOR>2.16)也是如此。所有区域的流行率均呈下降趋势;东部地中海地区的年度 AOR 范围为 0.84(95%CI,0.79-0.90),西太平洋地区为 0.97(95%CI,0.97-1.01)。汇总平均男女性流行率比为 1.00(95%CI,0.89-1.13)。敏感性分析证实了结果的稳健性。
在过去的 30 年中,梅毒流行率在全球范围内呈下降趋势。各区域之间的流行率存在很大差异,其中非洲区域始终受影响最大。