Korenromp Eline L, Mahiané Guy, Rowley Jane, Nagelkerke Nico, Abu-Raddad Laith, Ndowa Francis, El-Kettani Amina, El-Rhilani Houssine, Mayaud Philippe, Chico R Matthew, Pretorius Carel, Hecht Kendall, Wi Teodora
Avenir Health, Geneva, Switzerland.
Avenir Health, Glastonbury, Connecticut, USA.
Sex Transm Infect. 2017 Dec;93(8):599-606. doi: 10.1136/sextrans-2016-052953. Epub 2017 Mar 21.
To develop a tool for estimating national trends in adult prevalence of sexually transmitted infections by low- and middle-income countries, using standardised, routinely collected programme indicator data.
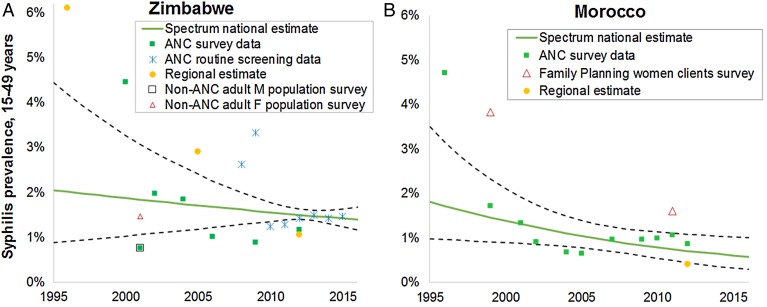
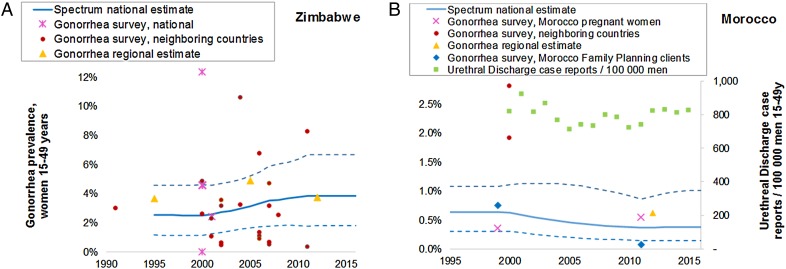
The Spectrum-STI model fits time trends in the prevalence of active syphilis through logistic regression on prevalence data from antenatal clinic-based surveys, routine antenatal screening and general population surveys where available, weighting data by their national coverage and representativeness. Gonorrhoea prevalence was fitted as a moving average on population surveys (from the country, neighbouring countries and historic regional estimates), with trends informed additionally by urethral discharge case reports, where these were considered to have reasonably stable completeness. Prevalence data were adjusted for diagnostic test performance, high-risk populations not sampled, urban/rural and male/female prevalence ratios, using WHO's assumptions from latest global and regional-level estimations. Uncertainty intervals were obtained by bootstrap resampling.
Estimated syphilis prevalence (in men and women) declined from 1.9% (95% CI 1.1% to 3.4%) in 2000 to 1.5% (1.3% to 1.8%) in 2016 in Zimbabwe, and from 1.5% (0.76% to 1.9%) to 0.55% (0.30% to 0.93%) in Morocco. At these time points, gonorrhoea estimates for women aged 15-49 years were 2.5% (95% CI 1.1% to 4.6%) and 3.8% (1.8% to 6.7%) in Zimbabwe; and 0.6% (0.3% to 1.1%) and 0.36% (0.1% to 1.0%) in Morocco, with male gonorrhoea prevalences 14% lower than female prevalence.
This epidemiological framework facilitates data review, validation and strategic analysis, prioritisation of data collection needs and surveillance strengthening by national experts. We estimated ongoing syphilis declines in both Zimbabwe and Morocco. For gonorrhoea, time trends were less certain, lacking recent population-based surveys.
利用标准化的常规收集的项目指标数据,开发一种工具来估计低收入和中等收入国家成人性传播感染的全国流行趋势。
“性传播感染频谱模型”通过对来自产前诊所调查、常规产前筛查以及可用的一般人群调查中的患病率数据进行逻辑回归,拟合活动性梅毒患病率的时间趋势,并根据其全国覆盖率和代表性对数据进行加权。淋病患病率通过对人群调查(来自该国、邻国和历史区域估计数)进行移动平均来拟合,此外,尿道分泌物病例报告也为趋势分析提供了信息,前提是认为这些报告的完整性相当稳定。利用世界卫生组织最新全球和区域层面估计中的假设,对患病率数据进行诊断测试性能、未抽样的高危人群、城乡和男女患病率比的调整。通过自助重抽样获得不确定区间。
在津巴布韦,估计梅毒患病率(男女)从2000年的1.9%(95%置信区间1.1%至3.4%)降至2016年的1.5%(1.3%至1.8%),在摩洛哥从1.5%(0.76%至1.9%)降至0.55%(0.30%至0.93%)。在这些时间点,津巴布韦15至49岁女性的淋病估计患病率分别为2.5%(95%置信区间1.1%至4.6%)和3.8%(1.8%至6.7%);摩洛哥分别为0.6%(0.3%至1.1%)和0.36%(0.1%至1.0%),男性淋病患病率比女性患病率低14%。
这一流行病学框架有助于数据审查、验证和战略分析,有助于国家专家确定数据收集需求的优先级并加强监测。我们估计津巴布韦和摩洛哥的梅毒患病率持续下降。对于淋病,时间趋势不太确定,因为缺乏近期基于人群的调查。